A comprehensive understanding of cerebral venous anatomy is critical for safe and effective neurosurgical procedures. In this study, we reconstructed, validated, and analyzed 3D MRA-based images of the superficial cerebral venous system in 100 individuals without intracranial pathology, focusing specifically on the VOL. We assessed its number, entry point, diameter, lateralization, and drainage patterns. To our knowledge, this is the largest cohort study to date examining VOL anatomy in an East Asian population.
The definition and number of VOLs
The inferior anastomotic vein, namely the vein of Labbé (VOL), is the largest anastomotic channel connecting the SMCV venous system with the TS, SPS, or SDA. Its importance during neurosurgical operations has been well reported. However, various definitions of the VOL were described in the literature [13,14,15]. Avci et al. defined VOL microsurgically as the inferior anastomotic vein connecting the SMCV territory to the TS or tentorial sinuses, and in the case of two superficial temporal bridging veins of equal diameter, these veins were found in 20% of the specimens, and treated as separate temporal bridging veins rather than a single duplicated VOL [18]. In contrast, other studies reported by Silva et al. and Sakata et al. described the case of two superficial temporal bridging veins of equal diameter as duplication of the VOL [16, 21]. Silva et al., using angiographic data, reported VOL duplication in 31% of cases, predominantly on the left side [16]. In a cadaveric series, Avci et al. found a clearly defined VOL in 80% of specimens, with 20% exhibiting two superficial temporal bridging veins of equal diameters [18]. Koperna et al. similarly reported a single VOL in 82% and double VOLs in 18% of cases, while Sakata et al. observed VOL duplication in 1 of 20 cadavers [21, 22]. These studies, however, were largely conducted in Caucasian populations, raising questions about their applicability to Asian cohorts.
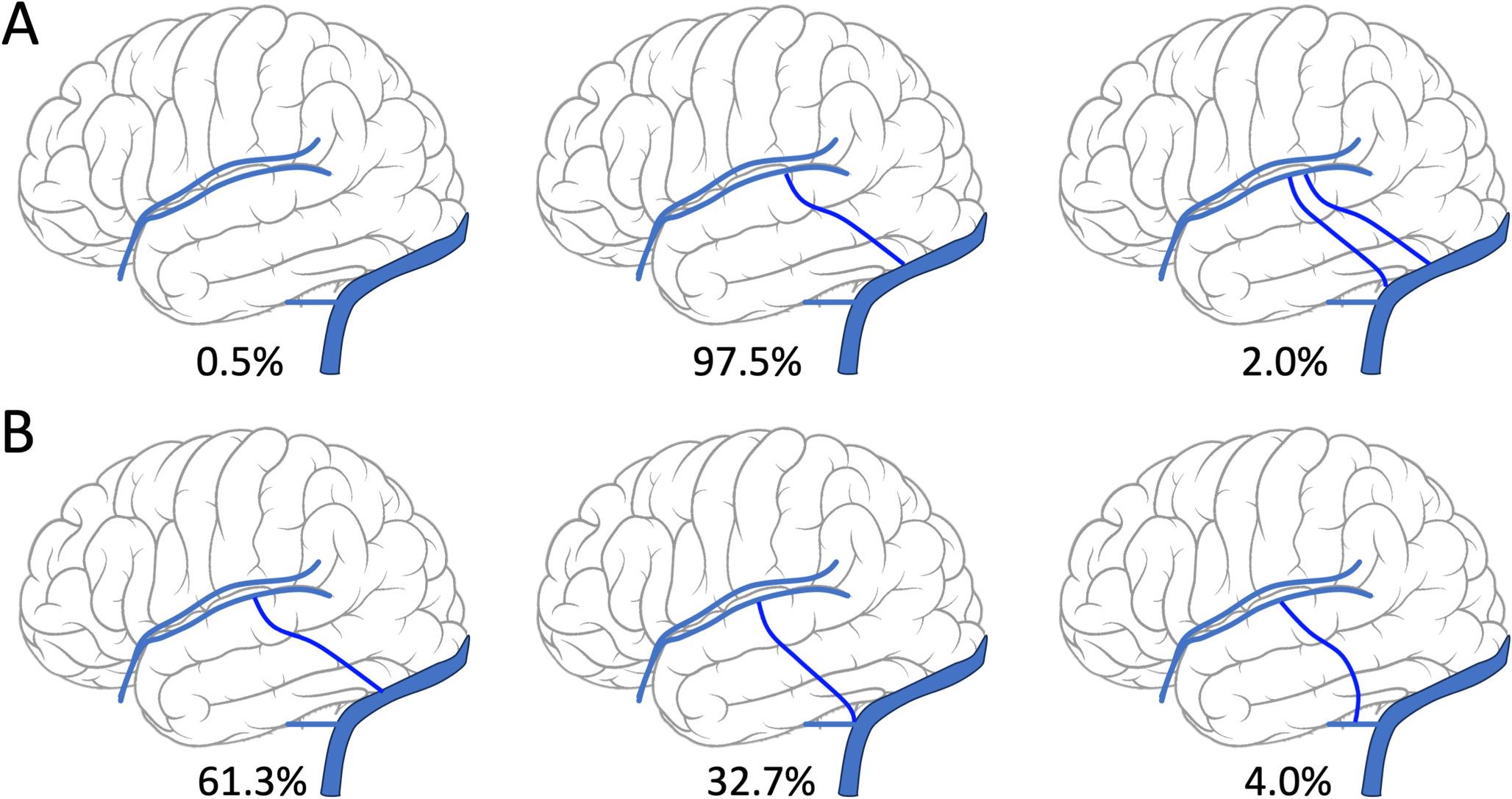
In this study, we defined the VOL, namely the inferior anastomotic vein, as the dominant lateral temporal bridging vein arising from the SMCV territory in the Sylvian region and coursing posteriorly and inferiorly to drain into the TS, SPS, or SDA. In the case of two dominant superficial temporal bridging veins of equal diameter, we adopted the definition of Silva et al. and Sakata et al. and described these veins as VOL duplication [16, 21]. Herein, VOL duplication was identified in 2% of hemispheres (4 of 200), suggesting a lower prevalence of this variant among East Asians. This difference may reflect true ethnic variation in cerebral venous anatomy. However, additional factors such as imaging modality, age, and venous thrombosis could also influence observations of the VOL’s anatomy. Different imaging modalities like CT angiography, MRA, and DSA yield varying detection rates for vein of Labbé duplication and drainage patterns due to differences in spatial resolution and flow sensitivity [19]. Therefore, we performed a validation by analyzing the MRA and DSA results from 10 patients, which yielded comparable results. Additionally, the development of VOL evolves postnatally, and neonatal venous thrombosis might appear as hypoplasia or absence on later imaging [23]. Thrombosis of VOL in adult could mimic absence and might be underdiagnosed, further confounding the analysis of VOL anatomy and requiring longitudinal analysis with searial imaging or age-stratified data [24].
Duplication of VOL may affect the surgical strategy in neurosurgical operation and neuroendovascular intervention. During subtemporal or transpetrosal surgical approaches, the VOL and associated temporal bridging veins may restrict temporal lobe mobilization [25]. Sacrificing either bridging vein would potentially result in venous infarction or intracerebral hemorrhage [26]. In cases of VOL duplication, selectively sacrificing one limb while preserving the other may improve surgical exposure with reduced risk. Our findings support the hypothesis that previously observed ethnic differences in posterior fossa venous anatomy, which may extend to superficial veins such as the VOL [27]. Further, during transvenous neuroendovascular interventions, occlusion of duplicated or variant VOL may cause cerebral edema or parenchymal hemorrhage [28]. Duplicated or variant VOL was associated with increased risks during transvenous stenting or angioplasty for TS stenosis by potentially impairing cortical venous drainage [28, 29]. In transvenous embolization of dural arteriovenous fistula, migration of embolic agent into cortical drainage poses significant risks if variants drain critical temporal lobe regions [30]. These variations may prompt protective strategies such as balloon-protected stenting or embolization, underscoring variant-specific intervention planning [29].
VOL entry points
The VOL typically drains into the TS, SPS, or the SDA. In a cadaveric study, Avci et al. reported direct drainage into the TS in 46.5% and indirect drainage via tentorial sinuses in another 46.5%, with only 7% draining into the SPS [18]. Fang et al. found TS drainage in 90–96% of individuals across multiple imaging modalities, and Ikushima et al. reported TS drainage in 80% and SPS in 4% [17, 31]. In contrast, we observed TS drainage in only 61.3% of hemispheres. Some possible reasons could explain this finding. First, earlier studies may have included SDA drainage under TS, whereas we categorized SDA entry points separately, accounting for 32.7% of cases [17, 31]. When combined, TS and SDA entry points accounted for 94%, aligning more closely with previous findings. Second, the higher SDA drainage may reflect ethnic anatomical variation in our East Asian cohort. Third, sampling biases, potential bias from imaging modality, and undiagnosed venous thrombosis remained potential confounders [24, 28]. Nevertheless, this study represents the largest imaging-based assessment of VOL entry points in an East Asian population to date.
VOL diameter and lateralization
In a study involving 60 cadaveric dissections, Fang et al. reported a mean VOL diameter of 2.8 mm, while Silva et al. reported 3.2 mm using angiographic data [16, 17]. In our cohort, the mean VOL diameter was larger: 3.77 mm in females and 3.87 mm in males. This discrepancy may be attributed to postmortem tissue shrinkage caused by formalin fixation or technical limitations of angiography, such as suboptimal contrast timing [32, 33].
Regarding the lateralization of VOL, Silva et al. reported left-side dominance in 45% and right-side dominance in 33% of hemispheres [16]. Di Chiro et al. similarly observed left-sided VOL predominance in 55% of individuals, and Ikushima et al. reported left dominance in 41% and right in 25% [31, 34]. Our results corroborate this trend, with the left VOL generally larger than the right. These finding might be explained by the embryological development of the cerebral venous system and asymmetric regression of primitive the embryonic tentorial sinus (ETS) [16, 19]. During fetal stages around 20 weeks, VOL forms as an anastomosis between middle and inferior cerebral veins, draining posteriorly via ETS into the marginal sinus [16]. Postnatal asymmetrical ETS regression significantly contributed to the determination of VOL course and led to left-sided VOL dominance and differential growth of the TS [19].
VOL-VOT relationship
The VOL and VOT are the principal venous outflows of the lateral cerebral surface, typically draining into the TS and SSS, respectively. Their relative size reflects drainage dominance: a VOL/VOT ratio > 1 implies TS dominance, whereas a ratio < 1 indicates SSS dominance [35]. Careful preservation of the dominant draining veins is required to avoid venous complications. In a study of 101 hemispheres, Silva et al. observed equal VOL and VOT sizes in 19% of hemispheres, VOL dominance in 31%, and VOT dominance in 50% [16]. Tomasi et al. further categorized venous dominance into five types based on VOL, VOT, and superficial middle cerebral vein relationships: type I with a dominant VOT (21.4%), typ II with a dominant VOL (16.7%), typ III with a dominant superficial middle cerebral vein (42.9%), typ IV with codominant veins of the VOT and VOL with a weak superficial middle cerebral vein (14.3%), andtype V with a direct connection between the VOT and VOL without a connection with the superficial middle cerebral vein (4.7%) [36]. Altough those studies did not assess lateralization, our data revealed a pattern of VOL dominance on the left and VOT dominance on the right. This asymmetry may reflect lateralized venous drainage patterns and has implications for personalized surgical planning.
Clinical relevance
Our findings underscore the significant variability in VOL anatomy. Given its pivotal role in cerebral venous drainage, the VOL, particularly the dominant one, should be preserved during neurosurgical and neurointerventional procedures. In cases where sacrifice or occlusion is unavoidable, careful planning and intraoperative navigation are essential to minimize the risk of venous infarction or hemorrhagic complications. Moreover, potential ethnic anatomical differences must be considered when extrapolating surgical strategies developed in Western populations to East Asian patients.

Comments (0)