
Remember me
Grade IV commercially pure titanium disks (5.0 mm diameter × 2.0 mm thickness), presenting either machined or sandblasted acid-etched (SA) surfaces, were manufactured by Implacil de Bortoli Implants (Santana de Parnaíba, SP, Brazil). To evaluate the mechanical, hydrophilic, and cytotoxic properties of the surfaces, the disks were divided into four experimental groups (n = 5 per group): Machined titanium disks without UV irradiation (control); Machined titanium disks irradiated with UV light for 30 min; SA titanium disks without UV irradiation; SA titanium disks irradiated with UV light for 30 min.
Ultraviolet irradiationSamples were exposed to UV light emitted by LED lamps (3 W, 365–385 nm wavelength range, 5.400 J) for 30 min using a custom-built prototype device (Fig. 1A, B). UV intensity was monitored throughout the experiments to ensure consistent exposure among all samples. Following irradiation, the disks were sterilized using gamma radiation.
Fig. 1
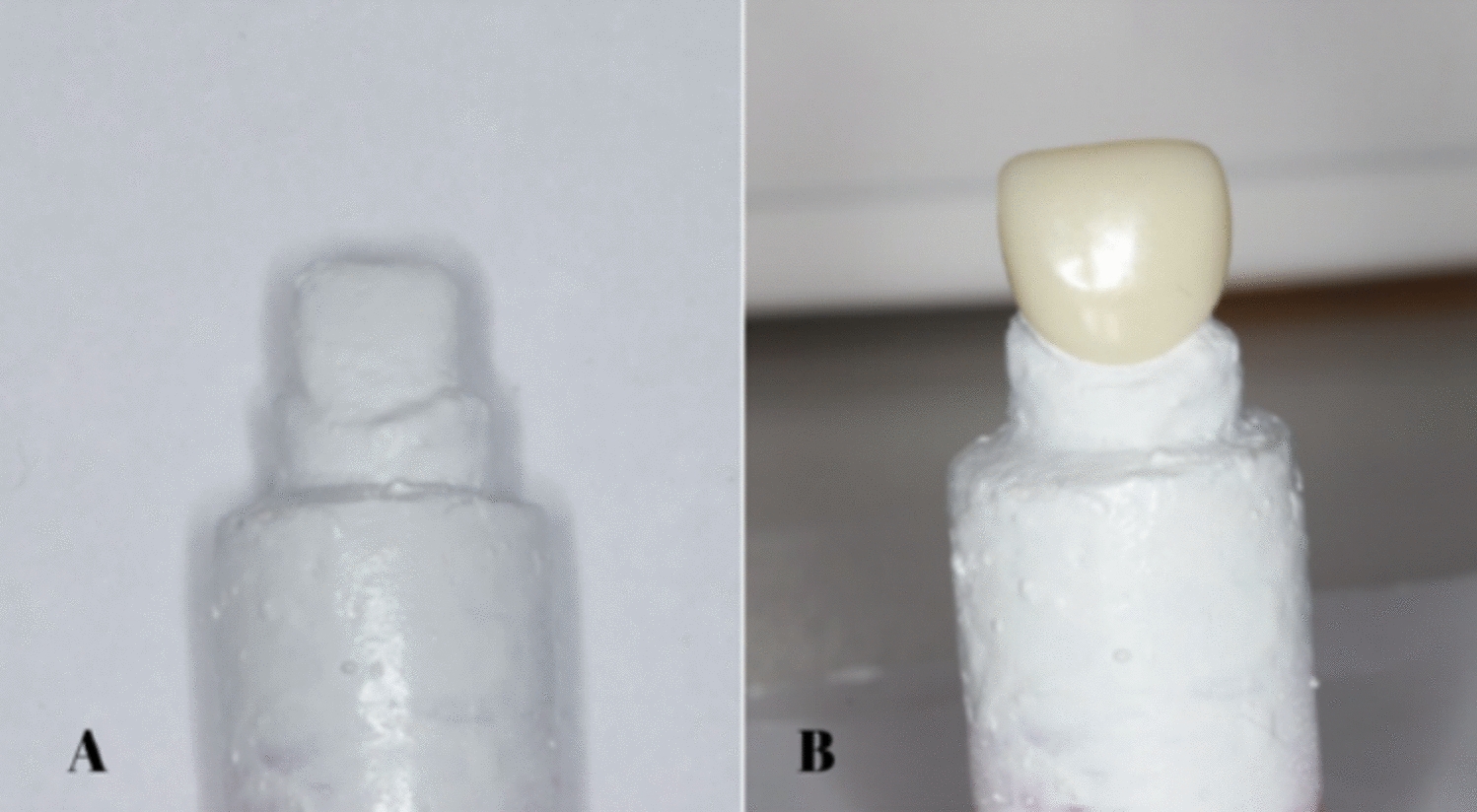
A Device containing ultraviolet (UV) light-emitting lamps. B Device with the lid closed and a safety mechanism that automatically stops UV emission. C Grade 4 commercially pure titanium dental implant (Implacil de Bortoli, Morse taper platform) irradiated with UV light for 5 min prior to clinical installation
Contact angle measurement (wettability test)Surface wettability was determined using a Ten Angstrom F100 goniometer. A 1 μL droplet of deionized water was placed on each surface, and the contact angle was measured with FTA32 Video 2.0 software. Surfaces with contact angles below 90° were classified as hydrophilic, whereas those above 90° were considered hydrophobic.
Roughness measurements (Ra/Rq)Three disks per group were examined to evaluate surface roughness (Ra and Rq). The profile of each group was determined by interferometry using the NewView 7100 equipment (Zygo UMI 807). Three measurements were taken and the roughness of each group was determined.
Ultrastructural analysis (scanning electron microscopy)Three disks from each sample were used for structural analysis. The samples were observed using a QUANTA FEG 250 FEI Eindhoven Scanning Electron Microscope (SEM), Netherlands, to observe the topography and morphology of the samples. The 1000 × and 5000 × increases were standardized.
Cell cultureMouse pre-osteoblastic MC3T3-E1 cells were obtained from the American Type Culture Collection (ATCC, VA, USA). Cells were cultured in alpha-modified Minimum Essential Medium (α-MEM) supplemented with 10% fetal bovine serum (Cultilab®, Campinas, SP, Brazil) and 1% antibiotic–antimycotic solution (Sigma, St. Louis, MO, USA). All procedures were conducted under a laminar flow hood to maintain sterility. Cultures were incubated at 37 °C in a humidified atmosphere containing 95% air and 5% CO₂.
Cell proliferation assayCell proliferation was assessed using the trypan blue exclusion method. Cultures were (2 × 104 per well) evaluated after 24, 48, and 72 h of incubation on the titanium disks. Cells were enzymatically detached using trypsin–EDTA solution (LGC, Brazil), centrifuged, and resuspended in 1 mL of fresh medium. A 10 μL aliquot of the suspension was mixed with 10 μL of trypan blue solution, and viable and non-viable cells were counted under an inverted phase-contrast microscope (Nikon Eclipse TS100) using a Neubauer hemocytometer (Fisher Scientific, Pittsburgh, PA, USA).
Cell viability (MTT) assayCell viability was determined using the MTT assay, which quantifies the metabolic reduction of yellow tetrazolium salts [3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide] to purple formazan crystals by mitochondrial dehydrogenases in viable cells.
Cells (2 × 104 per well) were seeded in 96-well plates and evaluated after 24, 48, and 72 h of culture (n = 5) at 37 °C. After incubation, 10 μL of MTT solution (5 mg/mL, Sigma Aldrich, USA) diluted in serum-free DMEM were added to each well and incubated for 3 h at 37 °C. The final concentration of MTT used was 0.5 mg/ml in the serum-free medium. Subsequently, 100 μL of 10% dimethyl sulfoxide (DMSO) were added to dissolve the formazan crystals. Optical density (OD) was measured at 590 nm using a microplate reader (ELX800, BioTek Instruments, Inc.).
Type I collagen quantification by ELISACells (2 × 104 per well) were seeded in 96-well plates and evaluated after 24, 48, and 72 h of culture (n = 5) at 37 °C. Type I collagen secreted by osteoblastic cells cultured on the different surfaces was quantified using enzyme-linked immunosorbent assays (ELISA) in a standard 24 well TC-plate (Sarstedt, Germany) sterile/DNA/DNase/RNase/Pyrogen free/non-cytotoxic. Supernatants were collected and centrifuged at 5000 × g for 15 min at 4 °C. Aliquots were analyzed following the manufacturer’s instructions (ALPCO, Salem, NH, USA). Samples were plated according to experimental group and time point, and 100 μL of detection antibody were added to each well, followed by 1 h of incubation at room temperature. Plates were washed with PBS containing 0.05% Tween 20, and 100 μL of streptavidin–peroxidase conjugate were added for 30 min of incubation at room temperature. After washing, 100 μL of tetramethylbenzidine (TMB) substrate were added and incubated for 15 min in the dark.
The reaction was stopped with 50 μL of 2N sulfuric acid (H₂SO₄), and absorbance was measured at 450 nm using a spectrophotometer (Epoch, BioTek, Winooski, VT, USA). Type I collagen concentration was expressed in picograms per milliliter (pg/mL). All experiments were performed in duplicate for each of three biological replicates.
Clinical trial—ethical aspects and study designThis study was approved by the Research Ethics Committee of the São Leopoldo Mandic Dental Research Center (CAAE #7.359.382). It was a single-center, prospective, interventional study. Statistical planning was based on previously published data [6], considering the critical value for the 95% confidence interval: 1.96, with a maximum acceptable deviation of 0.22 (22%), a minimum standard error of 5% of the mean (50%), and a significance level of p < 0.05, we arrive at n = 9.72, rounding to the next whole number; n = 10.
Ten participants of both sexes, aged 18–65 years, edentulous in the anterior maxillary region and in good oral health, were enrolled and treated between April and August 2025. All participants provided written informed consent after receiving detailed information about the study, in compliance with the 2020 CONSORT Statement. Exclusion criteria included pregnancy or lactation, systemic diseases affecting tissue healing, smoking, alcohol or drug abuse, uncontrolled diabetes, and use of medications interfering with bone metabolism.
Implant characteristics and data collectionA total of 20 Implacil de Bortoli sandblasted and acid-etched (SA) implants (Santana de Parnaíba, SP, Brazil), made of Grade IV commercially pure titanium with a Morse taper connection, were used. The sandblasting and acid-etching surface treatment was performed by the manufacturer according to a proprietary industrial protocol protected as a trade secret, therefore, specific parameters, such as particle size, acid composition, and processing conditions, are not publicly disclosed. All implants were supplied sterile and ready for experimental use. Ten SA implants were irradiated with UV light (96 W, 7 cm distance) for 5 min (total energy 28.800 J) immediately prior to placement without removing them from their sterile packaging (Fig. 1C). Implant dimensions were selected according to each patient’s clinical and anatomical requirements.
Preoperative evaluation included blood tests (glucose, complete blood count, coagulation profile) and cone-beam CT imaging for surgical planning. Each patient received two implants, one subjected to UV irradiation and one non-irradiated control, randomly assigned to opposite sides of the maxilla.
Surgical procedure and medication protocolPatients received 2 g of amoxicillin one hour before surgery. Facial antisepsis was performed with 4% chlorhexidine, and a 0.12% chlorhexidine mouth rinse was used for one minute. Local anesthesia was achieved with 2% lidocaine containing 1:100,000 epinephrine (Alphacaine®, DFL, Rio de Janeiro, Brazil). A crestal and intrasulcular incision was performed to elevate a full-thickness mucoperiosteal flap. Following standard drilling according to the manufacturer’s recommendations, implants were placed bilaterally in the maxillary canine region, corresponding to the replacement of the right and left maxillary canines.
SmartPeg transducers were connected for primary stability measurements, followed by placement of healing abutments. Interrupted sutures were made with 5–0 nylon (Ethicon, Johnson & Johnson, São José dos Campos, SP, Brazil) and removed after 14 days.
Postoperative medication included amoxicillin 500 mg every 8 h for 5 days, dexamethasone 4 mg every 24 h for 2 days, ibuprofen 600 mg every 8 h for 3 days, and 0.12% chlorhexidine mouthwash twice daily for 10 days. Patients received verbal and written postoperative care instructions.
Resonance frequency analysis (RFA)Implant stability quotient (ISQ) values were measured using the Osstell device (Osstell, Gothenburg, Sweden) with SmartPeg number 16, compatible with the Morse taper implants used. The first measurement was performed immediately after implant placement (T0), and subsequent measurements were taken every two weeks until the day 70 postoperative. SmartPegs were torqued to 10 N/cm [7]. Data were recorded for subsequent statistical analysis.
Statistical analysisParametric data were analyzed using two-way ANOVA followed by Bonferroni post hoc tests to compare differences between groups and time points. The normality of the clinical data were evaluated using D’Agostino–Pearson omnibus (K2). The significance level was set at p < 0.05. GraphPad Prism 10.4.1 software was used for statistical calculations and graph plotting.
Comments (0)