
Remember me
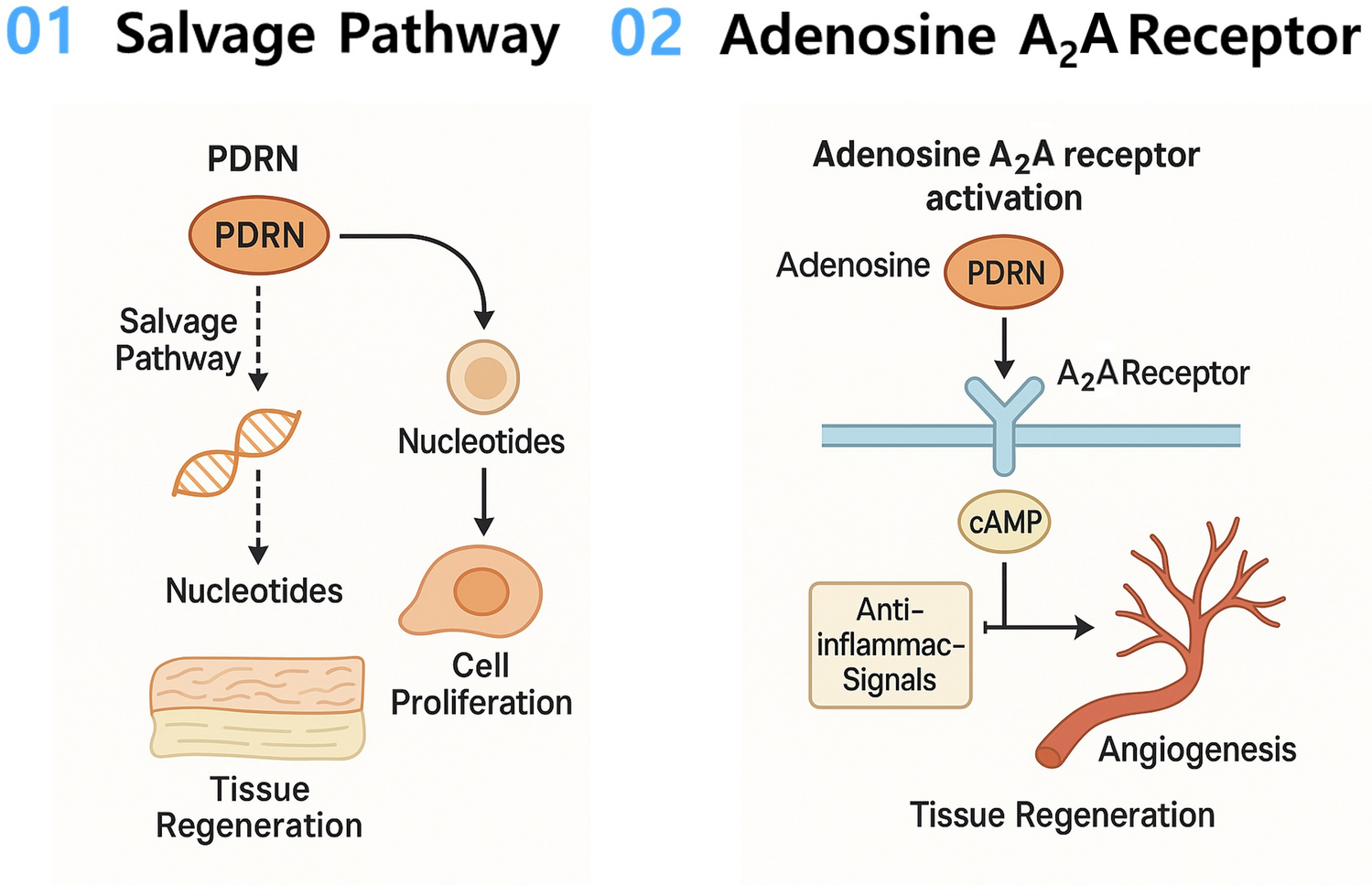

PDRN’s therapeutic effects in tissue regeneration are primarily achieved through two mechanisms: (1) the salvage pathway, and (2) activation of adenosine A2A receptors (Fig. 1). First, through the salvage pathway, PDRN’s degradation products serve as a source of nucleotides for cells, promoting DNA synthesis and cell proliferation in damaged tissues. In other words, by recycling nucleotides—the building blocks of nucleic acids (DNA and RNA)—cells conserve the energy and resources that would be required to synthesize new nucleotides de novo [16]. Adenosine, a nucleoside originating from PDRN breakdown, interacts with purinergic P2X and P2Y receptors (P2XR and P2YR), adenosine A2A and A2B receptors, and nicotinic acetylcholine receptors (nAChR) to regulate cellular and tissue functions, thereby stimulating pathways for proliferation, differentiation, maturation, and anti-inflammation [16]. Moreover, PDRN has been shown to modulate key signaling cascades in a mechanism analogous to adenosine. It suppresses the nuclear factor kappa B (NF-κB) pathway and activates the Wnt/β-catenin pathway, modulating the inflammatory response and playing an immunomodulatory role in tissue regeneration [17].
Fig. 1
Schematic diagram of the mechanisms of PDRN in tissue regeneration. PDRN acts via two main pathways: (1) Salvage pathway activation, whereby PDRN is broken down into nucleotides that are recycled for DNA/RNA synthesis in repairing cells. This conserves cellular energy by reutilizing nucleotide building blocks, accelerating DNA repair, cell proliferation, collagen synthesis, and bone formation. (2) A2A receptor activation, which increases cAMP and triggers signaling cascades that suppress inflammation and promote angiogenesis.
2.1 Salvage pathway and nucleotide supplyIn parallel with receptor-mediated effects, PDRN contributes to tissue regeneration through the “salvage pathway” of nucleotide synthesis [1]. PDRN is a mixture of double-stranded DNA fragments approximately 80–2200 base pairs in length, which are depolymerized by endogenous DNases into free purine and pyrimidine nucleosides and bases [18]. These liberated bases are then reutilized by cells to synthesize new DNA and RNA without expending the energy required for de novo nucleotide synthesis [9, 18]. PDRN’s nucleotide supply via the salvage pathway is particularly important under conditions of cellular stress or injury (e.g., hypoxia or trauma), when rapid cell proliferation is needed for healing. By using this energy-efficient salvage route instead of the ATP-intensive de novo pathway, cells in damaged or ischemic tissues can more readily achieve DNA repair and replication, thus accelerating tissue repair. PDRN breakdown products effectively support the replication of fibroblasts, osteoblasts, and other reparative cells, enhancing tissue turnover and wound healing. For example, providing exogenous deoxyribonucleotides has been shown to mitigate DNA damage and promote cell survival in ischemic or UV-damaged tissues [8, 9, 18, 19]. This salvage pathway is less energy-consuming and more efficient under conditions of cellular stress, which are commonly observed in inflamed or surgically injured oral tissues.
2.2 Adenosine A2A receptor activationPDRN is also known to act as a selective agonist of the adenosine A2A receptor, a G protein–coupled receptor widely expressed on immune cells, fibroblasts, and endothelial cells [1]. As PDRN is broken down by nucleases, the resulting adenosine molecules can bind to A2A receptors on cells such as fibroblasts [2, 20]. A2A receptor engagement leads to an increase in intracellular cyclic AMP (cAMP) and activates downstream signaling cascades that orchestrate an anti-inflammatory and pro-regenerative response. Specifically, A2A activation by PDRN suppresses the production of pro-inflammatory cytokines (e.g., tumor necrosis factor-α, interleukin-6) while increasing anti-inflammatory signals [21]. Concurrently, PDRN’s agonism of A2A receptors upregulates factors like vascular endothelial growth factor (VEGF), angiopoietin-1, and matrix metalloproteinase-2, all of which facilitate neovascularization in healing tissues [11]. This receptor-mediated mechanism enhances new blood vessel formation and modulates the inflammatory milieu, creating a more favorable environment for tissue healing [12]. Moreover, PDRN’s activation of A2A receptors has been shown to reduce NF-κB pathway activation and apoptosis in injured cells, thereby accelerating the resolution of inflammation. It downregulates key inflammatory mediators including IL-1β, TNF-α, inducible nitric oxide synthase (iNOS), and IL-6, while promoting tissue survival and repair [20, 22]. Importantly, the regenerative benefits of PDRN are abolished by A2A antagonists such as 3,7-dimethyl-1-propargylxanthine (DMPX), confirming that A2A receptor signaling is a primary pathway for its activity [18].
Notably, this dual mode of action—A2A receptor activation coupled with salvage pathway nucleotide provision—may confer PDRN a unique advantage over single-pathway agents. PDRN not only initiates pro-healing signaling cascades but also directly supplies the raw materials for nucleic acid synthesis in regenerating cells. This combination of signaling and substrate support underlies PDRN’s potency in stimulating the tissue repair in wounded, hypoxic, or ischemic environments for neural, skin, muscle and bone cells (Fig. 2) [23]
Fig. 2
Schematic summary of the representative signal pathways of polydeoxyribonucleotide (PDRN) for tissue regeneration. (Adapted from Oh et al., Biomaterials Research, 2025, CC BY 4.0 [23]) (A2AR, adenosine A2A receptor; A2BR, adenosine A2B receptor; ALP, alkaline phosphatase; α-SMA, α-smooth muscle actin; AMPK, AMP-activated protein kinase; AMP, adenosine monophosphate; AR, androgen receptor; ATP, adenosine triphosphate; BAX, Bcl-2-associated X protein; Bcl-2, B-cell lymphoma 2; BDNF, brain-derived neurotrophic factor; bFGF, basic fibroblast growth factor; cAMP, cyclic adenosine monophosphate; Col I, type I collagen; Col3, type III collagen; CREB, cAMP response element-binding protein; Epac2, exchange protein directly activated by cAMP 2; ERK, extracellular signal-regulated kinase; IL-1β, interleukin-1 beta; IL-6, interleukin-6; IL-10, interleukin-10; IL-12, interleukin-12; IL-13, interleukin-13; JAK, Janus kinase; JNK, c-Jun N-terminal kinase; MAPK, mitogen-activated protein kinase; MEK, mitogen-activated protein kinase kinase; nAChR, nicotinic acetylcholine receptor; NF-κB, nuclear factor kappa B; OPG, osteoprotegerin; P2R, purinergic receptor; P2XR, purinergic P2X receptor; P2Y2R, purinergic P2Y2 receptor; P2Y6R, purinergic P2Y6 receptor; pCREB, phosphorylated CREB; PKA, protein kinase A; RANKL, receptor activator of nuclear factor κB ligand; ROS, reactive oxygen species; RUNX2, Runt-related transcription factor 2; STAT3, signal transducer and activator of transcription 3; TCF, T-cell factor; TNF-α, tumor necrosis factor-alpha; VEGF, vascular endothelial growth factor)
2.3 Potential roles and recent advances in oral and maxillofacial tissue regenerationOne of the most promising applications of PDRN in dentistry is its role in osteogenesis and angiogenesis. PDRN has been shown to stimulate the proliferation and differentiation of osteoblasts, partly by increasing the expression of critical bone-forming genes such as RUNX2, osteocalcin (OCN), and osteopontin (OPN) [11]. By promoting a richer blood supply, PDRN ensures oxygen and nutrient delivery to regenerating tissues, which is crucial for oral wound healing and bone regeneration [24,25,26]. Activation of A2A receptors by PDRN markedly increases the expression of VEGF and other angiogenic factors (e.g., angiopoietin-1, MMP-2), thereby facilitating neovascularization in healing bone. Angiogenesis plays a pivotal role in early bone formation, coupling with osteogenesis to ensure successful tissue regeneration. In models of impaired healing such as diabetic wounds and ischemic flaps, PDRN significantly improved angiogenic markers (e.g., CD31, nitric oxide, angiopoietin levels) and accelerated wound closure [27, 28]. These findings underscore the importance of PDRN’s pro-angiogenic effect in supporting tissue repair.
PDRN also upregulates key osteogenic markers at the molecular level. RUNX2 is a crucial transcription factor in osteoblast differentiation [29]. Meanwhile, collagen type I alpha 1 (COL1A1) is an early marker of osteoblast differentiation; it is one of the first genes expressed when progenitor cells commit to the osteogenic lineage, making it a key indicator of the initial stages of bone formation [30]. Although RUNX2 and COL1A1 mRNA expression levels varied depending on the concentration of PDRN, the treatment generally influenced gene expression profiles associated with osteogenesis [31]. In vitro, mineralization and calcium deposition were enhanced in gingiva-derived stem cell cultures treated with PDRN, suggesting promotion of the later stages of bone formation [31]. Additionally, PDRN also promoted the growth of cultured human osteoblasts, accompanied by an increase in alkaline phosphatase activity, a marker of osteoblastic activity [24]. Through its pro-angiogenic and pro-osteogenic actions, PDRN creates a synergistic healing environment: new blood vessels support the maturing bone, and the forming bone secretes cytokines that further stabilize the vasculature. This combined action is especially beneficial in dental regenerative procedures (e.g., bone grafts, inflammatory diseases) where both revascularization and new bone formation are critical for success.
2.3.1 Bone graftConsidering PDRN’s synergy in promoting angiogenesis and osteogenesis, it can be significant potential for use in dental bone grafting procedures. Yun et al. introduced the concept of osteoimmunology, emphasizing that PDRN exerts its regenerative effects primarily through immunomodulation rather than direct osteogenic stimulation [32]. Specifically, PDRN activates the A2A adenosine receptor pathway, inducing a phenotypic shift of macrophages from the pro-inflammatory M1 type to the anti-inflammatory M2 type. This transition enhances the secretion of IL-10 and VEGF, suppresses TNF-α and other inflammatory cytokines, and establishes an immune environment conducive to angiogenesis, osteoblast activation, and bone remodeling. In 2021, Lim et al. reported in a New Zealand white rabbit model that applying PDRN at concentrations of ≥ 5 mg/mL on a block-type alloplastic scaffold resulted in significantly greater new bone formation at 8 weeks, comparable to the outcome achieved with 0.05 mg/mL of rhBMP-2 [13, 33]. To effectively utilize such hydrophilic agents, however, an appropriate scaffold capable of controlling the release profile in vivo is necessary [34,35,36]. Collagen sponge has received U.S. FDA approval as a carrier for rhBMP-2. More recently, demineralized dentin matrix (DDM), a type I collagen-based scaffold, has been highlighted as a bioactive carrier [35]. In 2016, PDRN successfully induced bone regeneration when combined with a DDM scaffold, suggesting its potential as a carrier system for clinical use [37]. The present review, however, limits its scope strictly to PDRN-related applications. Beyond preclinical feasibility, recent in vivo studies further support PDRN’s benefits in bone regeneration. Ko et al. conducted an in vivo study in beagle dogs undergoing alveolar ridge preservation procedures, demonstrating significantly higher bone volume and mineral density in PDRN-treated groups compared to controls [38]. Similarly, Lim et al. used a rabbit model of maxillary sinus floor elevation and observed enhanced new bone formation and greater vascularization in the PDRN group at both 2-week and 4-week intervals [39]. Furthermore, histologic analysis revealed that lateral sinus floor elevation augmented with PDRN led to earlier new bone formation and a higher bone-to-implant contact ratio, compared to conventional grafting alone [32, 40]. Although research is still limited on whether PDRN can exhibit osteoinductivity comparable to rhBMP-2 in clinical settings, its angiogenic, anti-inflammatory, and stem cell–stimulating properties are expected to be advantageous.
2.3.2 Temporomandibular joint disorder (TMD)It has been shown that PDRN can help prevent or attenuate numerous inflammation-related conditions, including bursitis of the shoulder and knee joints, fasciitis, and tendinitis [41,42,43,44,45,46]. PDRN may promote angiogenesis and tissue healing in osteoarthritic joints by down-regulating catabolic and pro-inflammatory mediators (such as tumor necrosis factor-α [TNF-α], interleukin-6 [IL-6], and high mobility group box 1 [HMGB1]) and up-regulating anabolic processes, as demonstrated in an in vitro model of osteoarthritis [47]. PDRN has been observed to modulate key inflammatory cytokines, including TNF-α, IL-1, IL-6, HMGB1, and IL-10, suggesting a potential regulatory role in controlling inflammatory processes. Notably, PDRN exerts its regenerative effects through the activation of adenosine A2A receptors, which modulates key inflammatory cytokines (TNF-α, IL-1, IL-6, HMGB1) and elevates anti-inflammatory cytokine IL-10, suggesting a broad regulatory role in inflammation. PDRN’s regenerative effects in musculoskeletal tissues are largely mediated through A2A receptor (ADORA2A) activation, which plays a critical role in cartilage and bone regeneration [42]. In vitro, PDRN has shown chondroprotective effects on cartilage cells, and in animal models of arthritis it significantly attenuated joint degeneration and inflammation compared to controls [48,49,50]. While in vitro studies have demonstrated chondroprotective effects of PDRN and animal models have shown significant attenuation of arthritis compared to controls, clinical studies on temporomandibular joint (TMJ) applications remain scarce. In 2024, Cenzato et al. reported 60 patients with TMJ osteoarthritis and conclude that pericapsular injection of PN and hyaluronic acid effectively reduces pain and improves mandibular kinematics [51]. Although PN and PDRN share structural similarities, their pharmacological properties are distinct. Because this review specifically focuses on PDRN, references to PN have been minimized to maintain clarity and consistency. Recently, prolotherapy using a combination of PDRN and hypertonic dextrose (10% d-glucose) has been reported as a beneficial treatment in TMD patients with TMJ osteoarthritis-related degenerative changes [52]. This regenerative injection approach aims to stimulate healing in ligaments and cartilage, and PDRN’s inclusion adds angiogenic and anti-inflammatory advantages. Additionally, PDRN has been shown to increase the proliferation of human preadipocytes, which could serve as a source of adult stem cells for tissue repair and regeneration [53]. These preadipocytes, when stimulated, have the potential to differentiate and contribute to the repair of musculoskeletal tissues, further supporting the therapeutic rationale for PDRN in TMD and other joint disorders. Recently, Choi et al. analyzed 66 patients with TMD who received prolotherapy with either hypertonic dextrose or PDRN [54]. They found that prolotherapy significantly improved pain and mandibular function, with the mean VAS score dropping from 4.34 ± 2.12 to 1.00 ± 1.58 and MMO increasing from 31.0 ± 8.7 mm to 40.8 ± 4.55 mm (p < 0.001). Both treatment groups showed comparable improvements, and 23 patients experienced complete resolution of joint noises, along with significant reductions in mandibular deviation. The authors concluded that prolotherapy—whether using PDRN or dextrose—is an effective intervention for improving pain and jaw function in refractory TMD patients. Similarly, Jang et al. evaluated 111 patients with TMJ osteoarthritis treated with prolotherapy on pericapsular space PDRN injections. They reported a significant reduction in pain (NRS 4.9 to 1.8) and an increase in mouth opening (32.6 ± 8.3 mm to 41.2 ± 5.7 mm; p < 0.001) [55]. Notably, 77.5% of patients showed clinically meaningful improvement on the PGIC scale, with greater benefits in acute cases and no adverse effects. Although PDRN demonstrates strong potential as a regenerative therapeutic agent in TMD and TMJ osteoarthritis, the optimal injection protocol—regarding dosage, frequency, and delivery site—has yet to be standardized. Further well-designed randomized controlled trials are warranted to establish the most effective treatment parameters and to validate the long-term safety and efficacy of PDRN-based prolotherapy.
2.3.3 Neurological symptomsNeuropathic pain, resulting from nerve injury or dysfunction of the somatosensory system, can severely diminish a patient’s quality of life because even innocuous stimuli (such as the touch of clothing) may cause persistent pain and discomfort. Various inflammatory substances have been found to induce astrocyte activation, which in turn promotes the development of allodynia, pain from normally non-painful stimuli [56, 57]. Considering PDRN’s anti-inflammatory actions, its potential to ameliorate neuropathic pain has been investigated. Lee et al. used a rat model of induced neuropathic pain to examine whether PDRN could reduce allodynia through anti-inflammatory effects [41, 58]. They found that local PDRN injections at the injury site significantly alleviated mechanical allodynia and decreased the expression of glial fibrillary acidic protein–a marker of astrocyte activation associated with neuroinflammation—in both a spinal nerve ligation model and a chronic post-ischemia pain model. This suggests that PDRN can mitigate neuroinflammatory responses and neuropathic pain symptoms following nerve injury.
Complex regional pain syndrome (CRPS), which can occur after peripheral nerve trauma, is characterized by severe burning pain, allodynia, and hyperalgesia, with symptom severity partly depending on the degree of sympathetic nervous system involvement [59]. Management of CRPS remains challenging, and many patients experience only partial or minimal symptom relief from current treatments. However, PDRN’s combined anti-inflammatory and angiogenic effects may offer a new therapeutic avenue. Activation of A2A receptors by PDRN leads to increased VEGF levels and enhanced endothelial cell migration and proliferation, improving tissue perfusion and healing. In 2016, the mechanisms of PDRN injection were highlighted as potential benefits for CRPS management, which could help alleviate symptoms by reducing inflammation and improving blood flow in affected tissues [60]. Thus, PDRN might serve as an adjunct or alternative in the treatment of CRPS, although clinical evidence in this specific context is still needed.
Traumatic neuropathies, nerve injuries caused by trauma or surgical procedures, do have an inherent capacity for regeneration, but recovery is often slow and incomplete. To improve recovery from peripheral nerve injuries caused by trauma or surgery, PDRN acts as a non-antigenic, non-toxic agent that strongly stimulates cell proliferation and wound healing, while also promoting angiogenesis [18, 61, 62]. It promotes Schwann cell and fibroblast proliferation, enhances wound healing, and stimulates angiogenesis in the injured nerve’s microenvironment. Improved blood supply is essential for delivering oxygen and nutrients to regenerating nerves, and PDRN’s pro-angiogenic effect likely contributes to a more conducive environment for nerve regrowth. Inflammatory cytokines such as IL-1 and IL-6, which can exacerbate nerve injury and edema, were found to be downregulated by PDRN treatment, leading to reduced swelling and secondary damage in injured nerves [63]. Studies have shown that PDRN treatment can accelerate neural tissue repair and functional recovery. Moreover, in a mouse sciatic nerve transection model, PDRN combined with VEGF (which PDRN is known to upregulate) produced superior regenerative effects [64]. In 2025, Sun et al. reported that PDRN and low-level laser therapy (LLLT) acted synergistically to enhance peripheral nerve regeneration in a crush-injured facial nerve model [65]. These findings suggest that PDRN could be a promising therapeutic for accelerating nerve regeneration and treating neuropathic pain following craniofacial nerve injuries—such as trauma to the inferior alveolar nerve—PDRN could be considered a promising therapeutic option to promote nerve regeneration and to manage neuropathic pain.
2.3.4 Inflammatory oral diseaseMost inflammatory conditions within the oral cavity originate from bacterial endotoxins released by biofilms. Biofilms accumulating on non-shedding surfaces—such as teeth, bone, and dental implants—require mechanical removal, as they are resistant to host immune responses and pharmacologic interventions [66, 67]. Peri-implantitis including periodontitis and medication-related osteonecrosis of the jaw (MRONJ) are two challenging oral conditions characterized by inflammation-driven bone loss and impaired healing. Contemporary treatment guidelines emphasize the effective decontamination and removal of these pathogenic biofilms and associated inflammatory and necrotic tissues.
MRONJ is also believed to originate from a state of drug-induced ischemia followed by antiresorptive or antiangiogenic agents [68]. Recent in vitro studies have demonstrated the potential of PDRN in mitigating such effects. PDRN has shown cytoprotective effects in macrophage cultures treated with zoledronic acid and lipopolysaccharide (LPS), where the combination of bacterial endotoxin and bisphosphonate synergistically reduced cell viability and increased inflammatory cytokine expression [22]. Notably, supplementation with PDRN significantly improved cell survival and downregulated inflammatory mediators. Jung et al. proposed that PDRN could serve as a valuable adjunct in MRONJ management by accelerating soft tissue healing and reducing the recurrence of osteonecrotic lesions [69]. Infection and inflammation have long been considered critical cofactors in the pathogenesis of osteonecrosis of the jaw (ONJ). Even when necrotic bone is exposed, lesions may remain asymptomatic if bacterial invasion does not occur. Conversely, inflammation and recurrence of MRONJ often follow surgical debridement if residual bone remains colonized by pathogenic bacteria [68, 70]. Hence, effective control of local biofilms has emerged as a crucial element in MRONJ therapy. Biofluorescence imaging devices have recently been introduced to detect and visualize bacterial biofilms intraoperatively, allowing for more accurate and complete debridement of necrotic tissues [70,71,72]. However, once inflammation has led to structural degradation of surrounding soft or hard tissue, merely removing the biofilm does not guarantee functional tissue restoration. It is well recognized that the healing capacity of the lesion is compromised if the surrounding supporting tissues have been destroyed [66]. In this context, PDRN—through its dual mechanism involving nucleotide salvage and adenosine A2A receptor activation—may suppress persistent inflammation while promoting tissue regeneration, thus reducing the risk of recurrence after treatment. Some studies support that PDRN’s ability to prevent osteonecrosis induced by both chemical (e.g., intra-articular monoiodoacetate injection) and mechanical insults (e.g., anterior cruciate ligament injury), as well as bisphosphonate exposure [73, 74].
These findings support the use of PDRN as a therapeutic adjunct in early-stage peri-implant mucositis and in “stage 0” MRONJ—that is, in patients who are at risk but hav
Comments (0)