
Remember me
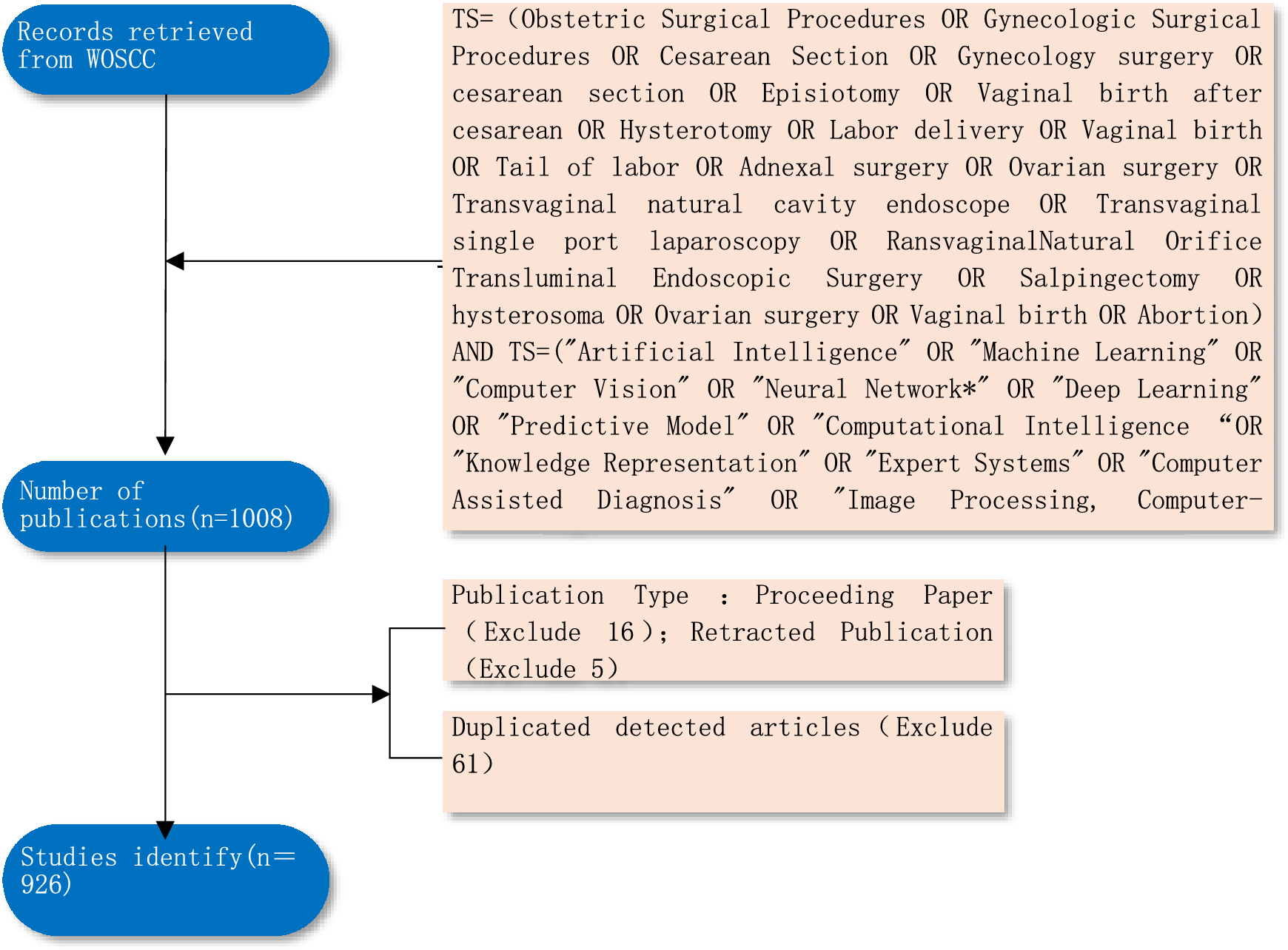
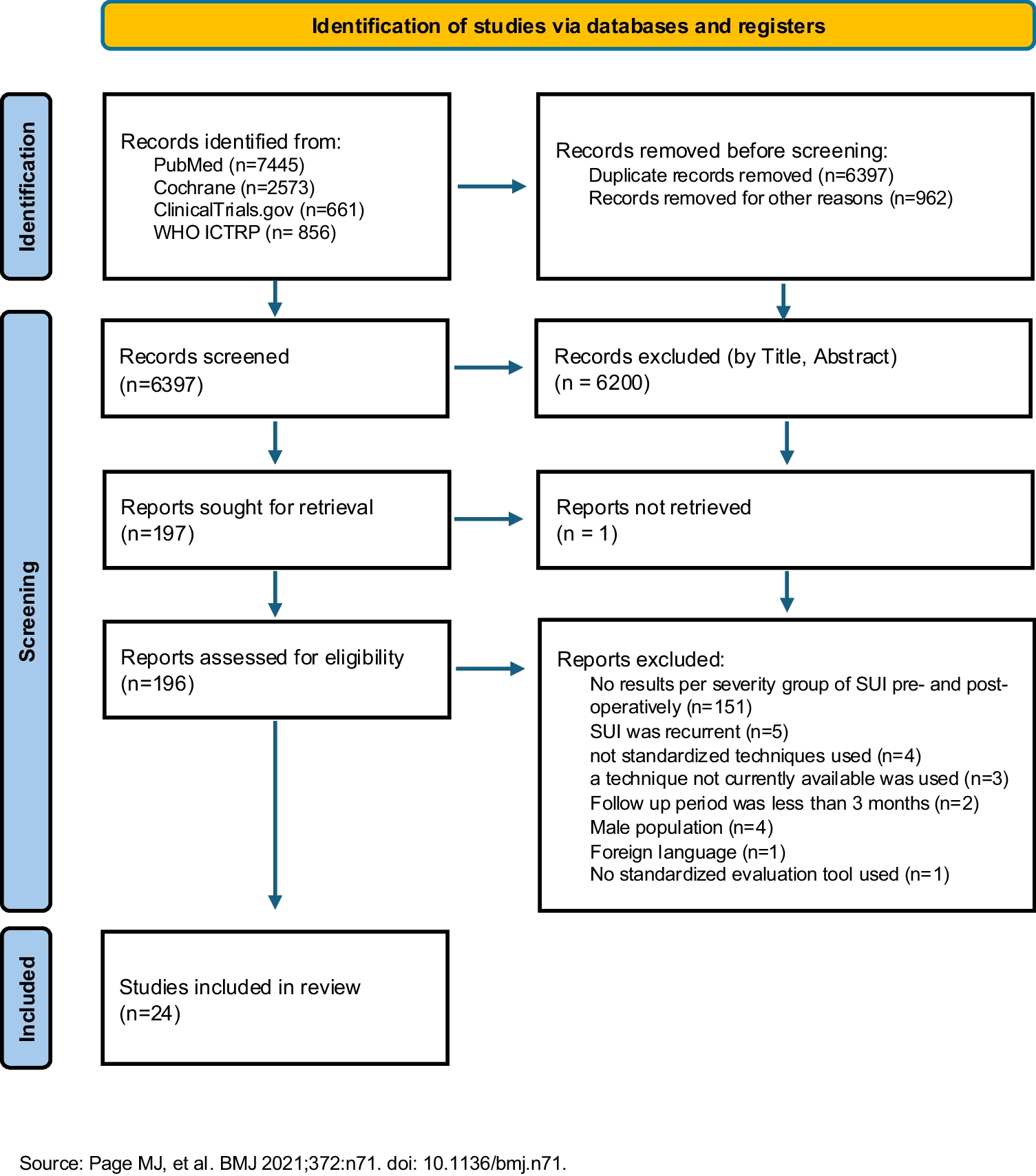
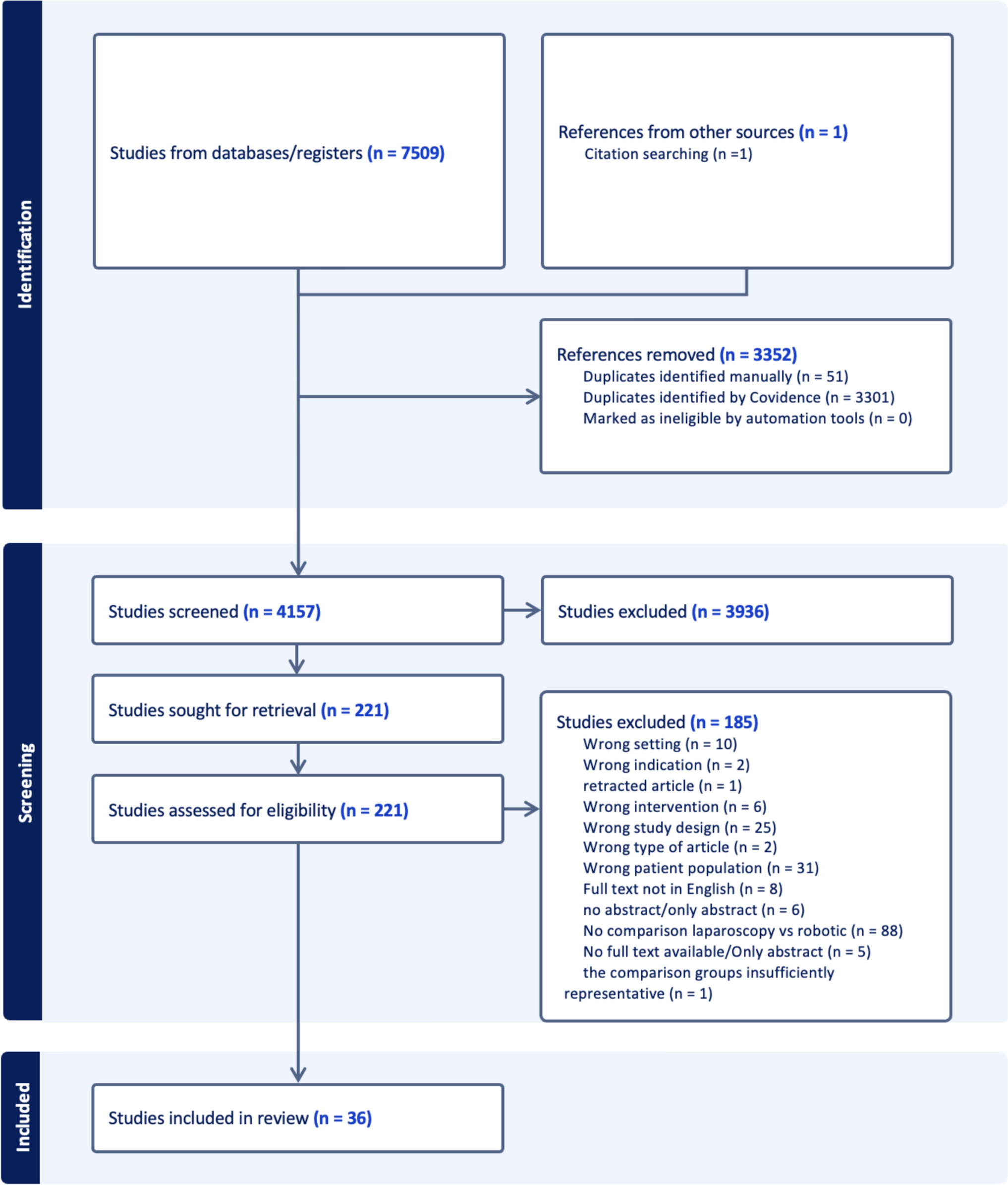
1508 records were retrieved using the described search strategy. Of those, 75 were identified as duplicate, leaving 1433 to be screened. During title and abstract screening 1263 records were excluded and 154 were excluded during the full text screening, leaving 16 records. In these 16 records it was stated that women with stage 1 uterine prolapse were included. However, the outcomes were not separately reported for this subgroup. Therefore, a request for research data was sent to the corresponding author of each study. Two corresponding authors (Oversand et al. & Eijsink et al.) responded to our outreach [19, 20]. Resulting in two studies eligible for analysis. From the 14 which were initially discarded, two only included patients with a stage 1 or 0 uterine prolapse. It was decided to also include these papers in the analysis even if their population also included women with a stage 0 uterine prolapse [21, 22]. The PRISMA flowchart of the search can be found in Fig. 1.
Fig. 1
Prisma flowchart of the performed systematic review
An overview of the papers included in this review is shown in Appendix 1. One paper was included in group 1 (i.e., prolapse surgery performed for stage 1 uterine prolapse). Two papers were included in group 2 (i.e., no surgery performed for stage 1 uterine prolapse). One paper was included in both groups, as some of the patients with a stage 1 uterine prolapse underwent hysteropexy and others did not. The quality of the papers and the bias domains with at least a moderate change of bias are summarized in Table 2.
Table 2 The quality of the included studies, assessed through the LEGEND scoring method and the bias categorized according to the bias domains defined in the Cochrane handbook for systematic reviews of interventions [17, 18].The longitudinal study from 2018 performed by Oversand et al. was included in group 1 [19]. They included 153 patients scheduled for treatment of symptomatic anterior POP by means of the Manchester procedure. Patients were excluded if they previously received prolapse surgery or hysterectomy, or if an indication for a hysterectomy was present. 61 of the included patients had a stage 1 uterine prolapse. The results of the group with stage 1 uterine prolapse were not reported in the article. However, the corresponding author provided us with the number of recurrences in the apical compartment, defined as POP-Q stage >0. Eleven patients (18%) treated by means of the Manchester procedure suffered from a recurrence in the apical compartment at 1 year follow-up. The study quality was assessed through the LEGEND method as a longitudinal study, both scorers found the article to be of good quality.
The paper by Eijsink et al. included 25 patients with a stage 1 uterine prolapse [20]. The included patients at least received an anterior colporrhaphy. Of the 25 patients with a stage 1 uterine prolapse, 20 patients received concomitant hysteropexy and five patients did not. So, this paper could be included in group one and group 2. Due to the short follow-up period of 6 weeks, the researchers were unable to accurately report on recurrences. However, the symptomatic improvement was used for analysis. In the group with concomitant hysteropexy two patients (2/20) reported no improvement. In the group without concomitant hysteropexy one patient (1/5) reported no improvement. The study quality was assessed through the LEGEND method as a longitudinal study, both scorers found the study to be of good quality.
The two papers included in group 2 excluded patients with a concomitant uterine prolapse larger than stage 1. However, the study designs of the two papers differ in many aspects. The randomized controlled trial performed by Rudnicki et al. followed 78 women, who were older than 55 years, for 12 to 36 months after surgery [22]. The included patients had at least a stage 2 anterior compartment prolapse with or without a concomitant posterior prolapse, for which at least an anterior colporrhaphy was performed. Patients were ineligible to participate if they received previous pelvic or vaginal surgery, used corticosteroids, or had a history of genital or abdominal malignancies. Recurrence in any compartment (compartment specifics were not reported), defined as a POP-Q stage ≥ 2, were reported as 60.2 at 1-year follow-up and 58.8% at 3-year follow-up. Symptomatic recurrence was assessed by means of questionnaires (pelvic floor disability index), 32% of the patients reported a bulging sensation at follow-up. The study quality was assessed through the LEGEND method as a randomized controlled trial, both scorers found the article to be of good quality.
Bergman et al. included 731 women with an isolated ≥ stage 2 anterior compartment prolapse and 384 women with an isolated ≥ stage 2 posterior compartment prolapse [21] The authors did not specify whether a concomitant stage 1 apical prolapse or no apical prolapse was present. According to suture-type (rapid or slow absorption) used during surgery, they were divided into two cohorts. Follow-up was set at 12 months, and recurrence was defined as “sensation of vaginal bulging”. The authors report a 28% recurrence in the anterior colporrhaphy group and 20% recurrence in the posterior colporrhaphy group. The cause of the recurrence was not specified as no postoperative physical examination was performed. The study quality was assessed through the LEGEND method as a cohort study. After first assessment and discussion between the scorers the study was scored as a prospective cohort study of lesser quality.
A total of 36 gynecologists, of which 3 completed a fellowship urogynecology, and one gynecologist in training, with a special interest in urogynecology, responded to our request. A response rate is impossible to calculate, as the survey was shared on different platforms. The mean age of the respondents was 47 years old, with 11 years of gynecological work experience. The respondents work in a general hospital (10 (28%)), teaching hospital (23 (64%)) or in an academic hospital (3 (8%)).
The question regarding the POP-Q C-value and indication for uterine prolapse repair showed a great clinical practice variation. The responses can be found in Table 3.
Table 3 Responses to the question from which POP-Q C-level the respondents perform apical prolapse repair surgeryThree respondents reported that they solely use supine-based POP-Q measurements as the method to establish whether uterine prolapse surgery is indicated. All other respondents either include physical examination in standing position, physical examination in the operating room, or the patient’s preference as additional method to set the indication for uterine prolapse surgery. Of the respondents, nineteen (53%) reported that they always counsel for concomitant uterine prolapse surgery, when discussing a surgery for the anterior or posterior compartment, twelve respondents occasionally discuss a concomitant procedure, and five respondents only discuss a concomitant procedure when indicated.
Comments (0)