Postpartum Changes in Urination and Defecation
Analyses of keyword co-occurrence, clustering, and bursts revealed that stress urinary incontinence (SUI) and anal incontinence are among the most frequently studied and rapidly emerging topics in postpartum PFD research.
SUI refers to the involuntary leakage of urine from the external urethral orifice during a sudden increase in intra-abdominal pressure despite the absence of symptoms under normal conditions [17]. Its prevalence among postpartum women is as high as 26% [5]. While not posing a direct threat to life, SUI has a profound impact on patients’ social contact, work, and sex life, ultimately diminishing quality of life and contributing to psychosocial issues such as disease-related stigma, anxiety, and depression [18, 19]. Among these issues, discussions on anxiety and depression are often more visible, whereas stigma is easily overlooked, leading patients to deliberately conceal their conditions, avoid seeking medical care, and experience social isolation [20]. However, most existing assessment tools for urinary incontinence rarely incorporate stigma-related components. Specifically, an evaluation of 11 outcome measurement tools for urinary incontinence interventions revealed that six tools did not include any items related to shame, whereas the remaining five contained only minimal content addressing this dimension [21]. The disconnect between the psychosocial burden of postpartum SUI and the limitations of current clinical assessment tools suggests that existing measures may fail to capture the full scope of patients’ experiences. This gap may hinder the development of holistic, patient-centered intervention strategies.
In recent years, continuous prevention systems for urinary incontinence have been extended to cover both the antenatal and postnatal periods. Specifically, antenatal preventive measures centered on pelvic floor muscle training have been shown to effectively enhance pelvic floor strength and resilience, mitigate obstetric trauma to the pelvic floor, and reduce the incidence of postpartum urinary incontinence [22]. Moreover, early postpartum assessment of PFD, combined with individualized rehabilitation strategies, plays a critical role in the prevention and management of postpartum urinary incontinence [23, 24]. It is worth noting that some women who do not experience urinary incontinence after childbirth may still develop it after menopause, primarily because of a decline in estrogen levels, which leads to reduced elasticity and tone of the pelvic supportive tissues [25]. However, the current research on the continuum from the postpartum period to menopause remains limited, hindering the development of evidence-based strategies for long-term management.
Anal incontinence following childbirth, characterized by the involuntary loss of flatus or stool, is mainly attributed to trauma to the anal sphincter complex and associated nerve damage during delivery. The prevalence reported in the literature varies significantly, ranging from 7% to 74% [26]. A study showed that approximately 86% of women had not disclosed a history of anal incontinence and were identified after clinical screening [27]. This indicates that postpartum anal incontinence is largely underestimated by patients, highlighting a significant gap between actual disease burden and patient self-reporting.
Therefore, future research should focus on addressing the current limitations in three key areas.
(1)
Assessment tools should be optimized by incorporating sufficient items related to shame and embarrassment to enable a more comprehensive evaluation of both physiological symptoms and psychosocial status.
(2)
Life course–based studies spanning the postpartum period to menopause are warranted. For example, establishing continuous health records and conducting long-term follow-ups from childbirth to older age could provide robust evidence to support the long-term management of PFD.
(3)
The implementation of proactive screening mechanisms in clinical practice is essential to address the issue of underreporting among patients with anal incontinence due to stigma or other factors. Such an approach may help alleviate psychological burden and improve access to timely diagnosis and treatment.
Mode of Delivery: A Major Risk Factor for Postpartum PFD
A substantial body of evidence indicates that the mode of delivery is closely associated with the development of postpartum PFD. The stretching forces of the pelvic floor tissues during vaginal delivery, particularly as the fetus passes through the birth canal, can damage the muscles, fascia, and ligaments, significantly increasing the risk of postpartum PFD. The cumulative effect of such injuries is particularly evident in women with multiple vaginal deliveries, which further increases the risk of postpartum PFD [28]. In contrast, cesarean section can reduce direct trauma to the pelvic floor tissues to some extent; however, it does not completely eliminate the risk of postpartum PFD, as pregnancy itself exerts physiological effects on the pelvic floor [29]. It is worth noting that most existing studies have focused on the period between 6 weeks and 6 months postpartum, likely because this timeframe is considered the critical period for pelvic floor recovery. Research conducted at this stage provides important clinical evidence to support early intervention strategies [30, 31]. However, long-term follow-up studies with durations exceeding 5 years remain scarce, resulting in a lack of sufficient longitudinal data to determine whether postpartum PFD symptoms worsen, improve, or develop over time.
These findings underscore several key directions for future research:
(1)
To strengthen long-term follow-up studies aimed at elucidating the natural course of postpartum PFD and clarifying symptom trajectories over time.
(2)
To identify risk indicators and high-risk maternal profiles for pelvic floor injury, thereby enabling more accurate prenatal risk stratification and facilitating targeted early interventions to reduce the incidence of birth-related trauma.
(3)
To investigate and promote perineal protection techniques that minimize the risk of pelvic floor tissue stretching and tearing during labor, while ensuring maternal and neonatal safety.
Ultrasound: An Essential Tool in the Diagnosis of Postpartum PFD
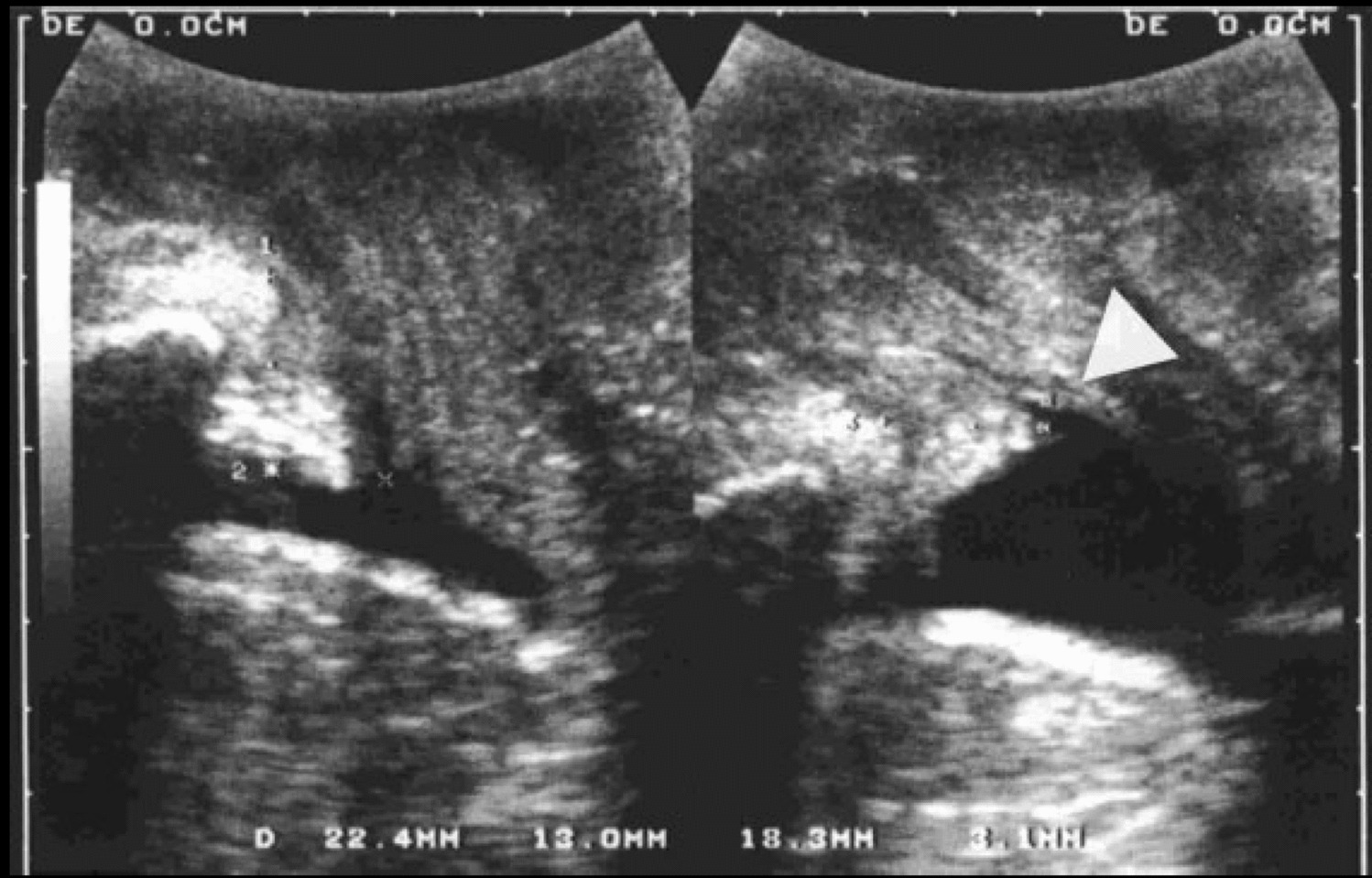
The results of keyword clustering analysis revealed a growing emphasis on the advanced utilization of imaging modalities in the study of postpartum PFD. Transperineal ultrasound, characterized by its noninvasiveness, dynamic capability, and high-resolution imaging, enables real-time assessment of both morphological and functional changes in the pelvic floor muscles. Specifically, it allows for the dynamic evaluation of the levator hiatus area, pelvic floor displacement, and sequential manifestations of pelvic organ prolapse [32]. Studies have confirmed that the thickness of the levator ani muscle, measured using transperineal ultrasound, is significantly negatively correlated with the incidence of postpartum urinary incontinence, whereas the degree of abnormal pelvic floor displacement shows a significant positive correlation with the severity of pelvic organ prolapse [33]. Recent studies have further confirmed that ultrasound examinations can detect pelvic floor support structural injuries at an early stage, particularly during the 42-day postpartum screening period, providing imaging-based evidence to guide the development of individualized rehabilitation strategies [33]. In addition, transperineal ultrasonography can effectively guide patients in performing proper pelvic floor muscle training. It provides real-time visualization of muscle movement direction, thickness changes, and organ positioning during contraction, thereby helping prevent incorrect contractions (e.g., bladder neck descent) or excessive straining [34, 35]. In clinical practice, it is recommended that ultrasound-based assessment parameters be used to dynamically adjust rehabilitation training programs, thereby enhancing the safety and effectiveness of pelvic floor muscle training.
Clinical practice should emphasize the combination of ultrasound assessment results with rehabilitation programs. Future research should focus on optimizing the quantitative ultrasound measurement system, systematically exploring the correlation between imaging findings and clinical symptoms, and actively promoting the application of artificial intelligence in automated analyses to enhance diagnostic accuracy and efficiency.
Postpartum Pain: An Emerging Research Focus
Postpartum pain can be categorized as acute or chronic. Although pregnancy- and delivery-related acute pain typically subsides over time, approximately 35% of women report persistent pain—referred to as chronic postpartum pain—between 8 months and 12 years after childbirth [36]. Chronic postpartum pain refers to a chronic pain syndrome that persists for more than 3 months after childbirth, primarily manifesting as localized or multisite pain. It mainly includes pelvic girdle pain, chronic pelvic pain, and perineal pain, with an incidence ranging from 1% to 18% [37]. It affects not only physical health but is also closely associated with psychosocial dysfunction. Clinical evidence suggests that the prevalence of anxiety and depression is significantly higher in women with chronic postpartum pain than in those without [38]. Its substantial impact on women’s long-term health and chronic postpartum pain remains under-recognized and under-addressed in clinical practice, largely owing to its lower prevalence than that of acute postpartum pain. A study conducted in 2022 found that health information related to chronic postpartum pain was often insufficient or inaccurate. Most women did not receive information regarding the possibility of persistent postpartum pain and were unaware of when and where to seek help [39]. On the basis of the current situation, future research should prioritize strategies to improve disease literacy among postpartum women, such as health education campaigns, evidence-based informational resources, and multimedia outreach. Additionally, developing and evaluating multidisciplinary interventions that incorporate rehabilitation medicine, psychological support, and other relevant disciplines may foster comprehensive biopsychosocial recovery after childbirth.
Growing Focus on Psychosocial Dimensions
In the keyword co-occurrence analysis, “quality of life” and “postpartum depression” appeared as high-frequency terms with 153 and 26 occurrences, respectively (Table 2). Notably, quality of life formed an independent cluster tag (#6), highlighting its central role in postpartum PFD research. Studies have shown that postpartum women with PFD report significantly lower quality of life scores than healthy postpartum women. In particular, symptoms such as urinary incontinence and pelvic organ prolapse often lead to social withdrawal, further exacerbating the psychological burden on affected individuals [40].
Keyword burst analysis further revealed that “postpartum depression” has remained a research hotspot since 2015. Postpartum depression is a depressive disorder that occurs during the postpartum period and is characterized by low mood, loss of pleasure, diminished interest, fatigue, reduced activity, and decreased energy. It has been reported to co-occur with PFD in up to 32% of cases [41, 42]. The physical discomfort caused by PFD may lead to decreased self-esteem and emotional disturbances, while depressive symptoms can further reduce patient adherence to rehabilitation, thereby creating a vicious cycle [43, 44].
Recently, increasing attention has been paid to the psychosocial aspects of PFD. Notable developments include the development of valid and reliable condition-specific quality-of-life questionnaires for women with PFD [45]; prevalence of anxiety and depressive symptoms and their association with PFD [46]; and effect of depression and anxiety on the success of pelvic floor muscle training for PFD [47]. However, current studies rarely include randomized controlled trials (RCTs) on psychological interventions for postpartum pelvic floor disorders (PFD) or longitudinal cohort studies conducted in low- and middle-income countries, resulting in a lack of relevant robust clinical evidence. Therefore, future efforts should focus on developing interdisciplinary interventions that integrate pelvic floor rehabilitation with psychological therapies. Greater emphasis should be placed on incorporating psychosocial factors into the rehabilitation process to promote holistic recovery across the physical, psychological, and social domains.

Comments (0)