
Remember me
We conducted a parallel-design randomized trial to evaluate an educational intervention aimed at reducing work-related screentime in healthcare workers. The trial was reviewed by the University of Nebraska Medical Center Institutional Review Board (Protocol # 514–21-EX) and classified as exempt (educational, behavioral, and social science research under 45 CFR 46:104(d), category 2). Participants provided electronic informed consent before enrollment. All procedures followed the ethical standards of the responsible committee and with the Helsinki Declaration. Research Electronic Data Capture (REDCap) [14] was used to communicate with participants and track data. The trial was registered at ClinicalTrials.gov (NCT05106647) on November 4, 2021, before the first participant was enrolled. This report follows Consolidated Standards of Reporting Trials (CONSORT) guidelines [15].
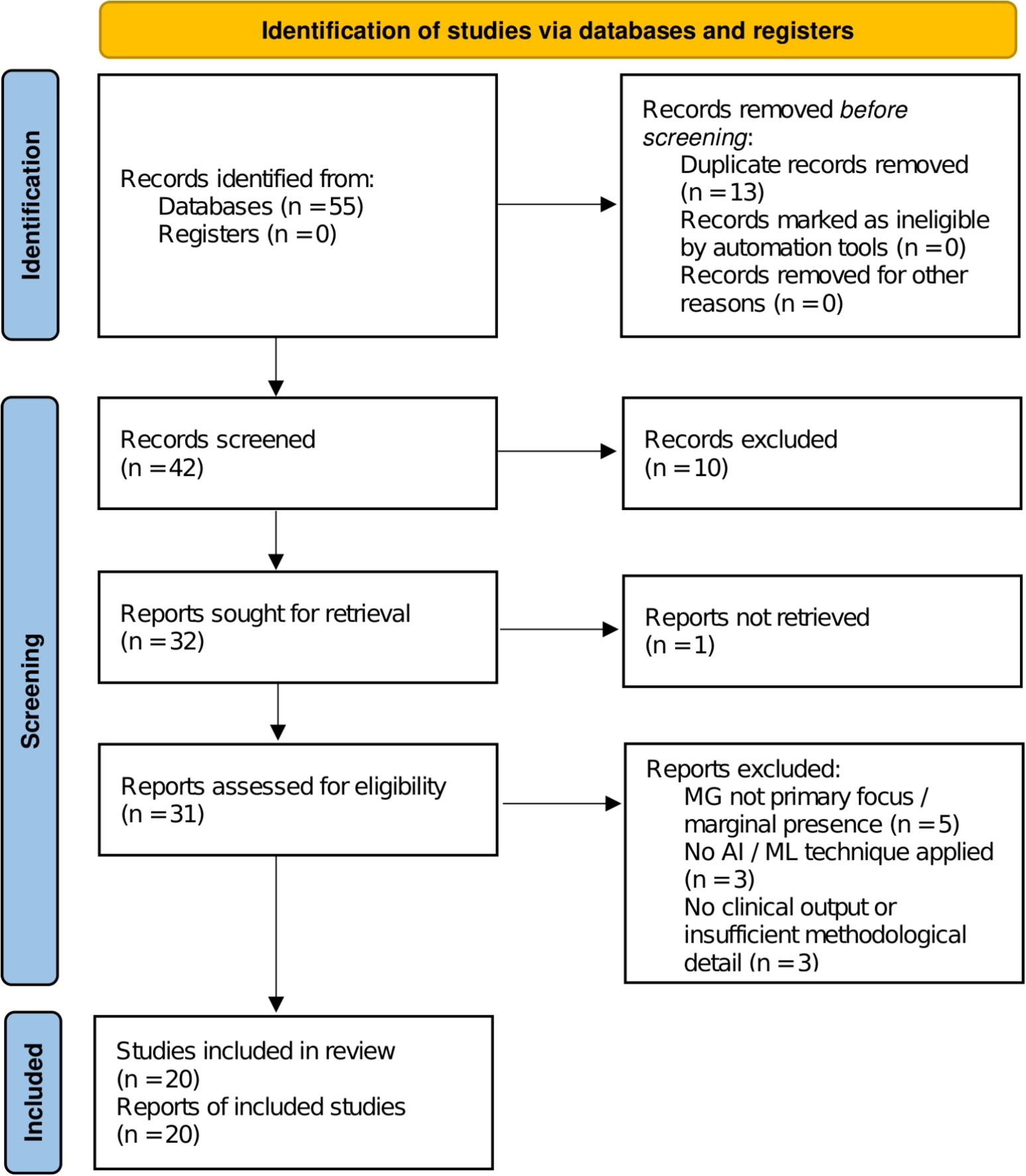
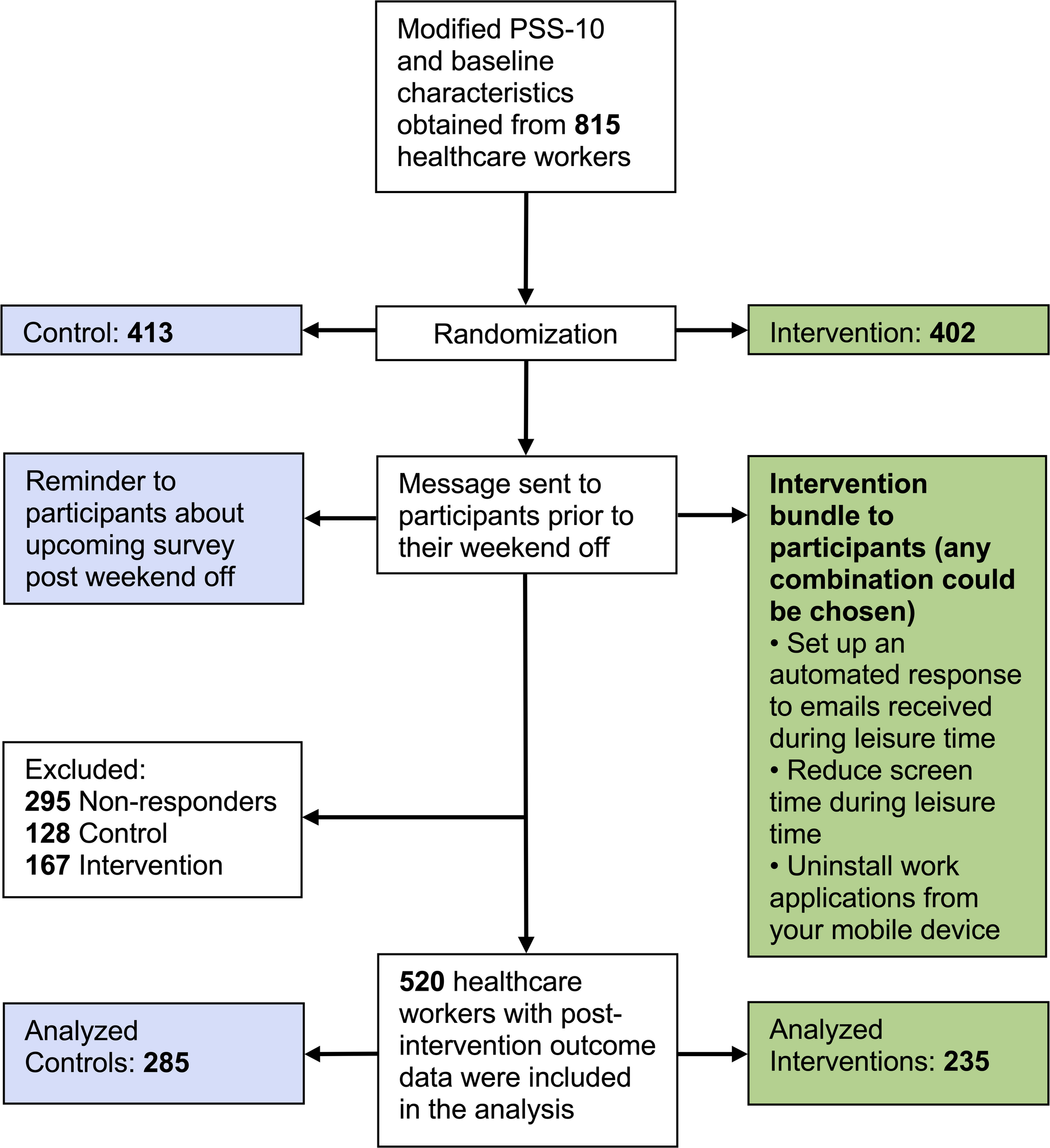
Study PopulationAdult healthcare workers who were able to read English, routinely used a smartphone, and had a work email application installed on their smartphone were eligible for enrollment. Coordinated from a United States academic anesthesiology department, participants were recruited using flyers, e.g., in the hospital cafeterias or at educational meetings, Quick Response (QR) codes embedded at grand rounds presentations, and a social media campaign (see Supplementary Information). From November 2021 to November 2023, we enrolled 815 healthcare workers (advanced practice providers, nurses, attending physicians, trainee physicians, and others), of whom 402 were randomized to our threefold educational intervention and 413 to no education. Among them, 295 did not respond to the post-intervention survey, so no outcome data could be collected. Our analysis set thus includes 520 workers, of whom 235 were assigned to the intervention, and 285 were assigned to the control (Fig. 1). The intake form included “other” categories for healthcare workers’ occupations other than advanced practice providers, nurses, and physicians (e.g., occupational, physical, and respiratory therapists, psychologists, or social workers). Similar to a hospital wellness program, ongoing participation was not mandated, and like most wellness programs, involvement was not compensated.
Fig. 1 Intervention
InterventionHealthcare workers were involved in the study's design by piloting the data collection tool and providing feedback on the choice of outcomes. Using the digital randomization function in the REDCap, participants were randomized 1:1 without stratification to our educational intervention or a reference group before a work-free weekend. The intervention group was provided the following threefold approach to reduce screen time during a selected weekend: 1) activate an automated response to emails received during leisure time, 2) reduce screen time during leisure time, and 3) uninstall work applications from personal mobile devices. The suite of interventions was presented through REDCap and virtual educational videos. Daily implementation of these interventions during the “off weekend” was strongly encouraged. Our education implementation strategy is informed by the COM-B model (Capability, Opportunity, Motivation-Behavior), which postulates that education interventions are most efficiently achieved through physical capability and reflective motivation [16]. Herein, we focused on increasing knowledge about the effects of screen time on well-being and offered the physical capability to have a work-free weekend. In the end, participants were free to follow all, some, or none of the threefold interventional strategies.
OutcomesOur primary outcome was participants’ post-intervention stress, adjusted for baseline stress. Stress was measured by the Perceived Stress Scale (PSS)−10, a 10-item self-report measure that is widely used to assess the degree to which life situations are stressful [17]. PSS-10 scores are consistent over time with repeated testing and are a reliable measure of psychological stress over various ages, education levels, and incomes [18]. The score ranges from 0–40, with higher values indicating worse stress [18].
The PSS-10 was administered to participants twice using REDCap infrastructure, once at enrollment and a second time on Monday after their trial weekend off. In case of non-response to the Monday message, participants received a daily reminder message for up to three additional subsequent days.
Our secondary outcome was average daily personal device screen time use during the trial weekend, adjusted for baseline screen time exposure. Based on feedback in preliminary testing, personal device daily screen use was not recorded in minutes but recorded from the reporting functions built into participants’ handheld devices and was reported on an hourly 11-point ordinal scale ranging from “0 to < 1 h” to “ > 10 h”.
Statistical AnalysisAnalysts were masked to group allocation until the primary analysis was complete. Given the nature of the study, participants could not be masked, but they were not informed whether we considered their assigned exposure intervention or lack thereof to be treatment versus control.
Analyses were performed using a modified intention-to-treat approach, with the modification being that participants with missing outcome data had to be excluded. The primary analysis, the effect of the intervention on stress, was performed by fitting a linear regression model with the assigned intervention group as the primary covariate and the post-intervention PSS-10 score as the outcome, adjusted for baseline PSS-10 scores. For the secondary analysis, the effect of the intervention on self-reported screen time was assessed by fitting an ordinal regression model with the reversed average post-intervention screen time as the outcome (so that a higher value corresponds to a lower average screen time) and the assigned intervention group as the primary covariate of interest, adjusted for reported baseline screen time. Exploratory analyses included the association between self-reported screen time and stress, which was assessed using a linear regression model, and the effect of the intervention based on which of the three interventions (activate an automated response to emails received during leisure time, reduce screen time during leisure time, and uninstall work applications from personal mobile devices) were adhered to. In line with the pragmatic design, participants randomized to the intervention group could choose to follow any combination or none of the suggested interventions, similar to other hospital wellness programs [19]. Given that the choice of which of the suggested screen-time limiting approaches to follow was left to the discretion of the participant in the intervention group, the exploratory analyses are observational in nature. Statistical significance was set at a level of P < 0.05. No multiple testing correction was applied, and thus, the non-primary analyses should be interpreted as exploratory in nature. All analyses were conducted using R statistical software (version 4.3.1; R Core Team 2023).
Based on a similar study, we assumed a baseline mean PSS-10 score of 20 with a standard deviation of 7 [20]. We defined a reduction in stress of 10% from baseline as clinically meaningful after the trial weekend, estimating a mean score of 18 and a standard deviation of 7 for the intervention group [21]. We estimated that 194 healthcare workers per group would provide 80% power for detecting a significant difference in PSS-10 score at an alpha of 0.05 using G-Power 3.1 [22].
Comments (0)