In this study, we developed and validated a novel computational framework for real-time HRV analysis, implemented in the software tool CODO Monitor. Our work addresses two of the most significant barriers to the clinical application of real-time HRV monitoring: high inter-individual variability and data contamination from procedural artifacts. The proposed methodologies—an adaptive alert algorithm, a manual artifact management system, and a multi-scale visualization approach—collectively enhance the robustness, personalization, and interpretability of HRV analysis in complex clinical environments.
A key contribution of our framework is the adaptive alert algorithm, which personalizes alert thresholds using the statistical distribution of each patient’s own data. As demonstrated in our results, physiological indices such as HR can vary significantly from population norms, and HRV metrics often exhibit non-Gaussian distributions. By employing an IQR-based method, our algorithm provides a statistically robust approach that accommodates these individual-specific and distributional characteristics. In practical terms, the three preset levels of α in our implementation can be interpreted as ‘sensitive’ (α = 1.724), ‘intermediate’ (α = 2.465), and ‘conservative’ (α = 3.207) alarm strategies. In our case-study dataset, decreasing α from 3.207 to 1.724 increased the fraction of alerts from 2.7% to 6.2% for the LF/HF ratio, illustrating the expected trade-off between sensitivity and the number of alerts. In clinical practice, α can therefore be chosen according to the desired balance between early detection of subtle changes and avoidance of alarm fatigue. This methodology represents a substantial improvement over conventional fixed-threshold systems, offering the potential to increase the specificity of alerts, reduce alert fatigue among clinical staff, and ultimately make real-time monitoring more clinically meaningful.
Furthermore, the manual annotation and exclusion mechanism directly confronts the challenge of data quality in real-world clinical settings. Procedural artifacts are an unavoidable reality of patient care, yet they can severely compromise the validity of HRV indices. Our results confirm that by enabling clinicians to exclude these contaminated periods from statistical calculations, the reliability of the personalized thresholds is significantly improved. This workflow-integrated approach to data cleaning is a practical and effective method for enhancing the robustness of real-time analysis, ensuring that clinical decisions are based on the patient’s underlying physiological state rather than on noisy, artifactual data.
The integration of these components within a multi-scale visualization platform transforms the system from a simple data monitor into a powerful tool for clinical interpretation and research. This is particularly significant in neonatal care. ECGs are noninvasive and provide continuous, real-time data, and previous studies have reported an association between autonomic dysfunction and severe infections in infants [25]. However, analyzing ECGs from very preterm infants has been challenging due to the difficulty in obtaining stable data amidst frequent nursing care and crying. Our framework addresses this specific challenge. The ability to reliably assess cardiac autonomic activity by excluding artifact-prone periods from noninvasive bedside monitor signals provides an extremely useful source of information for future neonatal care. Our framework was operationally validated at the bedside using ECG data from 24 newborn patients. This approach, enabling robust analysis even in a noisy clinical environment, is a major step forward in making real-time autonomic assessment a clinical reality.
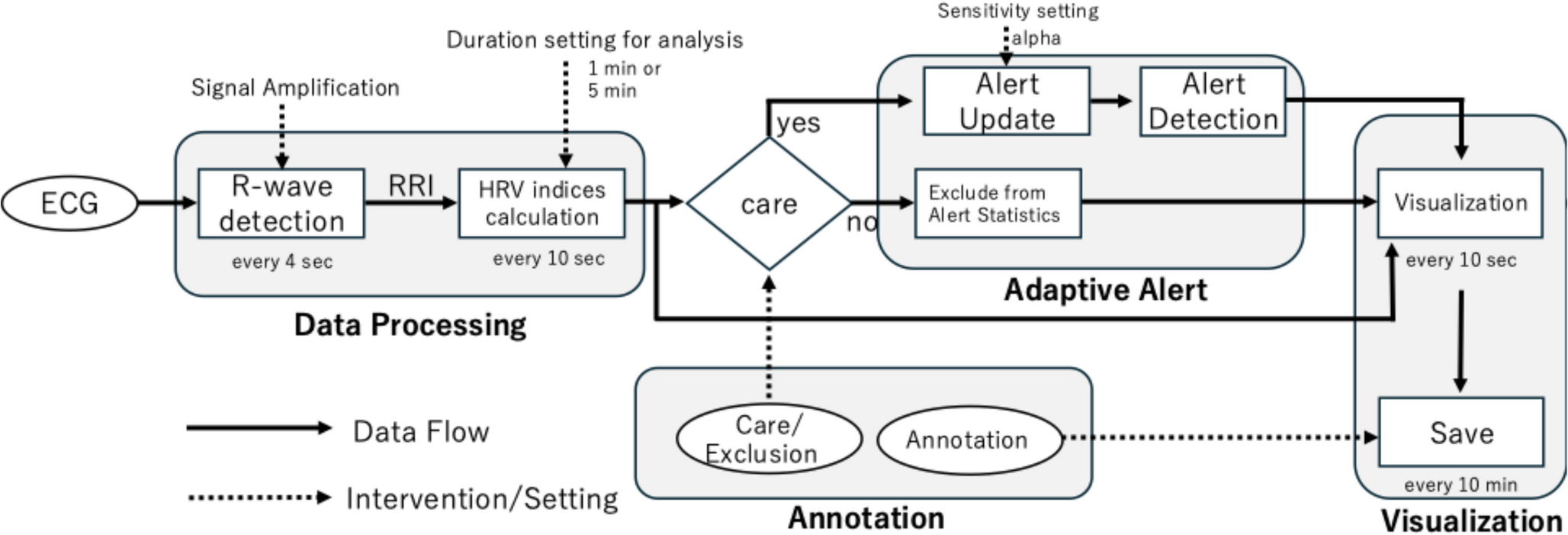
This study has several limitations. First, the accuracy of the entire analysis pipeline is fundamentally dependent on the quality of the input ECG signal and the reliability of R-wave detection. There are various methods for R-wave detection, and this study did not conduct a comprehensive comparative analysis. Exploring faster and more accurate methods remains a future challenge. However, as shown in Fig. 2, the current system handles both pediatric and adult data and demonstrates performance comparable to other R-wave detection methods. It also successfully detects R-waves in noisy conditions. Furthermore, data have been collected from 24 newborns, and experts in neonatal electrocardiography have reported no issues with the R-wave detection. While validated with such clinical data, the algorithm’s performance under conditions of extreme noise has not been exhaustively tested. Future work should focus on enhancing the signal processing front-end to improve robustness.
Second, the current implementation utilizes an analog signal input. While digital integration offers seamless data transfer, it is often hindered by manufacturer-specific proprietary protocols that restrict interoperability. By leveraging the standard analog output available on most major monitoring systems (e.g., Philips, GE Healthcare, Nihon Kohden), our framework achieves universal compatibility without requiring expensive, vendor-specific middleware. This design choice prioritizes immediate clinical applicability and accessibility across diverse hospital environments. While the analog approach ensures broad compatibility, future expansion to support direct digital data streams from hospital networks would further enhance integration capabilities.
Third, the care/data exclusion function and manual annotations of artifacts introduced in this system allow doctors and nurses to annotate during care and procedures, making it particularly useful for neonatal care with minimal burden. Because these annotations are time-locked to concrete clinical events, they serve a dual purpose: they define which periods should be excluded from learning the statistical baseline, and they also provide a structured record that links interventions (e.g., repositioning, suction, medication) to the subsequent evolution of HRV indices. This dual role is clinically important when interpreting whether a sudden change in autonomic activity is plausibly explained by ongoing care or may instead indicate emerging pathology. For this reason, we deliberately avoided purely automatic artifact rejection based solely on signal-quality metrics or waveform morphology. By restricting exclusion to periods that staff explicitly mark as care-related, the framework minimizes the risk of inadvertently removing genuine physiological instability while still protecting the adaptive thresholds from obvious procedural artifacts. However, this strategy requires staff intervention and cannot eliminate all non-care-related artifacts. Even though quartile-based statistics are less affected by outliers, explicitly removing artifacts further improves overall data quality. In particular, spontaneous crying, motion, or technical issues still need to be identified by staff, which can be burdensome in a busy NICU. Future work will be integrating automatic signal-quality indices and machine-learning–based suggestions for care/noise annotation to reduce this burden while preserving clinician control over which data are removed from threshold learning and clinical interpretation.
Several frameworks and software packages have been developed for HRV analysis. Representative research-oriented tools include Kubios HRV, RapidHRV, RR-APET, and the open-source spectral analysis toolbox by Rodríguez-Liñares et al. [17]. These packages support a wide range of time-, frequency-, and in some cases non-linear indices. CODO Monitor currently supports the following time-domain indices: pNN50, SDNN, RMSSD, and the SDNN/RMSSD ratio, non-linear indices of Poincaré plots: SD1, SD2, and SD1/SD2, and frequency-domain indices: VLF, LF, HF, and their ratios. The number of supported HRV indices is lower than that of Kubios HRV [14], widely used for HRV analysis, providing a broad set of time-, frequency-, and non-linear indices. Future work will include supporting other indices, including Higuchi fractal dimension, acceleration capacity and deceleration capacity.
On the other hand, most of systems support only offline post-hoc analysis. They are lacking real-time processing pipelines, explicit artifact-management mechanisms, and workflow-integrated user interfaces tailored to continuous bedside monitoring and clinical alert management. Systems that support monitoring HRV indices during acquisition include the mobile version of Kubios HRV, MemCalc, LabChart HRV, AcqKnowledge HRV, and OpenSignals. Kubios HRV mobile app offers real-time visualization and artifact correction. Nevertheless, its alert functions mainly target signal-quality issues rather than implementing personalized alarm algorithms that automatically optimize thresholds based on each patient’s statistical baseline. LabChart with HRV Module (ADInstruments, Dunedin, New Zealand), AcqKnowledge software (BIOPAC Systems, Inc., Goleta, CA, USA), and OpenSignals (PLUX Wireless Biosignals S.A., Arruda dos Vinhos, Portugal) are versatile physiological recording systems used with dedicated hardware. They either do not provide HRV-based alerting or, do not include an adaptive threshold. MemCalc/Win (GMS Co., Ltd., Tokyo, Japan) [26] supports real-time monitoring of time- and frequency-domain indices and has a track record of clinical use, yet it does not incorporate automatically adaptive, patient-specific thresholds or an artifact-management mechanism that is linked to manual annotations. In comparison, the proposed CODO Monitor uniquely integrates, within a single stand-alone software package, (i) an IQR-based adaptive threshold-learning algorithm that personalizes alerts for each HRV index using the patient’s own distribution, (ii) a workflow-integrated artifact-management scheme in which bedside procedures (e.g., nursing care) can be annotated with a single click and automatically excluded from the statistical computations in real time, and (iii) a multi-scale visualization module that simultaneously displays short-term (minutes) and long-term (hours) HRV dynamics. Thus, CODO Monitor is positioned as a “clinically integrated bedside solution for personalized and artifact-resilient real-time HRV monitoring,” filling a gap that is not addressed by existing open-source or commercial HRV tools.
Finally, while this paper establishes the technical and functional validity of our framework, large-scale clinical studies are required to verify its effectiveness in improving patient outcomes. Such studies remain a crucial objective for future research.
In conclusion, this paper presents a clinically-oriented framework that improves the practicality and reliability of real-time HRV monitoring. By systematically addressing the core challenges of personalization and artifact management, our methodology provides a robust platform for both clinical care and research. This work represents a significant step toward translating the potential of real-time HRV analysis into tangible improvements in vital sign management and patient outcomes.

Comments (0)