
Remember me
This study used the measure of ULY at age 50 and revisited the apparent contradiction of women’s longer life and more years spent in poor health, which has often been labelled a paradox. We found that at age 50 women spent more life years in poor health than men, and that these differences in ULY were primarily attributable to the mortality effect (ME), i.e., differences in women’s and men’s total number of life years. While the contribution of the ME to the total gender gap in ULY was consistently positive, the health effect (HE) was more variable between countries and health indicators, but in almost all cases smaller than the ME. Our findings align with previous decomposition studies showing that women’s longer survival is the dominant contributor to the gender gap in unhealthy life years: In Van Oyen et al. [39], Nusselder et al. [40], and Luy [41], the mortality effect consistently outweighed the health effect, which was smaller and also more variable across countries and health dimensions.
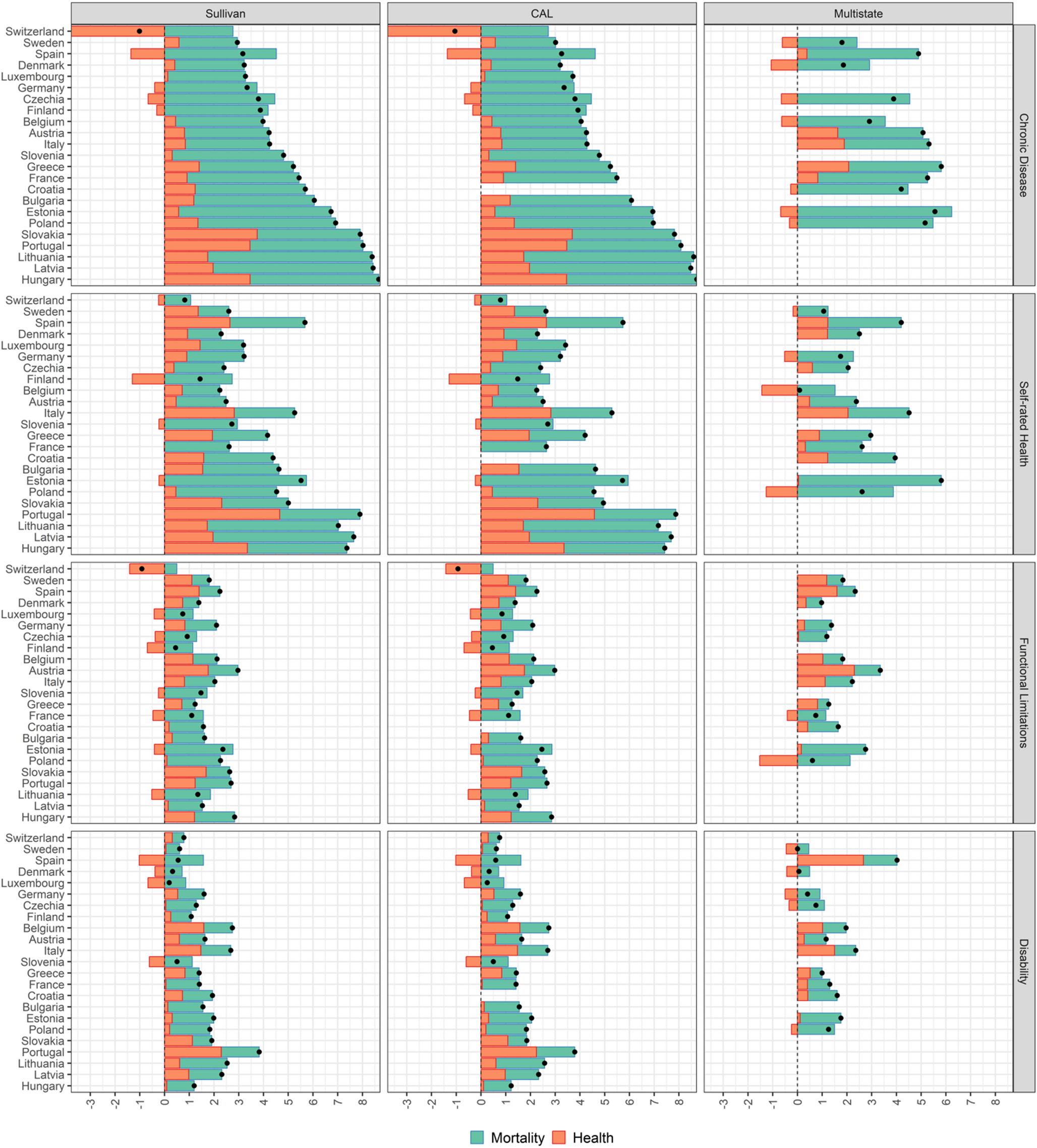
Fig. 2
Contribution of mortality to the gender gap in unhealthy life years at age 50 (female minus male) in four health dimensions and three estimation methods, in percent values. Negative contribution means that either the gender gap was positive or the contribution of the health effect was negative. In these cases, we plot contribution of mortality effect as 100%. Countries ordered by the gender gap in ULY for chronic diseases derived according to the Sullivan method.
Data Source: SHARE Waves 6 and 7 and Human Mortality Database (2024).
Greater effects of mortality on the total gender gap in ULY imply that women’s higher life expectancy is mainly responsible for their greater number of life years spent in poor health, offering support for the longevity hypothesis. Our results therefore confirm Luy and Minagawa’s [29] conclusion that “women suffer from worse health than men do not in spite of living longer, but because they live longer” (p.17).
Consistent with previous findings [6, 40,41,42], our study confirms further that the extent of the gender gap in ULY depends strongly on the health dimension analysed. We find that the differences between women and men in the number of life years spent in poor health tends to be large when health is defined according to chronic diseases and SRH, and comparatively small for functional limitations and disability. While the occurrence of this variation by health dimension has been repeatedly noted, the reasons for its variation remain an open question. Luy [41, 43] suggests that the main reason for this variation lies in the severity of the diseases underlying different health dimensions. The number of life years spent in poor health rises with total life years, and this increase in ULY is more pronounced when the mortality risk associated with poor health is lower. In modern societies, gains in life expectancy occur mainly at older ages. As the risk of health problems rises with age, such conditions accumulate and are more common in the oldest age groups—especially those conditions that do not necessarily increase mortality. In other words, because people typically spend more years with less severe than with critical health problems, the additional life years that distinguish populations with different life expectancies, such as women and men, are largely years lived with less severe conditions. These milder problems can more frequently be found in dimensions such as chronic diseases, whereas the causes of functional limitations and disability are generally linked to more serious health problems with a stronger relationship on mortality.
This explanation is consistent with the observation that the populations in our study can be divided roughly into two groups in terms of the extent of gender differences in ULY and its variation by health dimension: those with lower levels of life expectancy for both sexes and bigger gender gap in ULY, exemplified by some of the Eastern European countries (Croatia, Slovenia, France, Bulgaria, Hungary, Poland, Estonia, Latvia and Lithuania), and those with higher life expectancy and smaller gender gap in ULY (all others). In general, the longevity hypothesis is confirmed more clearly and across all health dimensions for the first group of countries. For the remaining countries, Switzerland, Sweden, Austria, Portugal, Spain, Italy, Greece, Slovakia, and Belgium, we observe similar results as for the first group for chronic conditions and SRH, but we find a less consistent picture for disability and functional limitations. Taken together, these results indicate that the larger the gender gap in ULY, the larger the ME. Note that the extent of the gender gap in ULY depends both on differences in life expectancy and on the health dimension considered.
There are some limitations to our study that need to be noted. First, it is important to stress that this study draws on broad health indicators, which may not be transferable to all health characteristics. In particular, many minor or specific illnesses with known gender differences are not reflected in the aggregated measures considered here. Therefore, our results do not rule out the possibility that there are specific diseases which occur more frequently and severely in women than in men.
Second, the decomposition of the gender gap in ULY into ME and HE provides insights into the effects on the total number of life years spent in poor health, but gives no details on the specific origins of the underlying processes, such as gender differences in age-specific mortality rates or transitions between health states. Instead, the applied decomposition isolates the separate contributions of two population-level components: life years lived, as determined by the age-specific mortality rates of the period, and the prevalence of poor health. This distinction is important because ULY is a population-level aggregate outcome measure and not a measure of the processes that determine these outcomes. While these two components are endogenous to each other - differential mortality by health status influences health prevalence, and health prevalence in turn influences total mortality - this endogeneity does not invalidate the decomposition. As long as we recognize this interplay and interpret the results as reflecting the effects of these two aggregate components rather than differences in the underlying processes, the conclusions drawn from such a decomposition remain valid.
Finally, as demonstrated by Muszyńska-Spielauer and Spielauer [44], the SHARE data applied in the study is subject to selective attrition on health and other characteristics that influence health, raising the possibility that our estimates of ULY may be biased. While younger individuals in good health are more likely to leave the predominantly longitudinal study sample, at older age it is individuals in the poor health that are more likely to attrite. Additional to health-selected attrition, as men are more likely to leave the longitudinal samples [45, 46], the differences between women and men in the prevalence of poor health are likely to be biased by attrition.
Conversely, our study also has important strengths. To the best of our knowledge, this is the first study to explore the mechanisms behind the relationship between life expectancy and years spent lived in poor health by gender using such broad cross-national coverage and a wide variety of health indicators and methodological approaches to estimate ULY. These strengths increase the robustness of our results and conclusions, thereby advancing our understanding of the mechanisms underlying the gender gap in ULY in European countries.
Comments (0)