The impact of light and moderate exercise on cardiovascular health has been extensively examined in health literature [46,47,48], whereas strenuous PA (both high intensity and high volume of exercise) has not been explored to the same extent. Prior to this study, examinations of relevant literature have resulted in a scientific statement review, meta-analysis and guideline recommendations pertaining to the association between heightened PA and cardiovascular health/mortality [8, 9, 27]. These reviews concluded that the benefits associated with PA would far outweigh the risks for the majority of those in the general population, whilst also not confirming a threshold for when the lifespan could be compromised [9, 49]. Our comprehensive review of relevant literature synthesises and critically evaluates evidence on the impact of strenuous exercise on the risk of adverse cardiovascular-related events and mortality which enables a more balanced assessment of evidence as previous reviews did not adequately explore the implications of PA classifications and measurements, timeframes, outcome and relevant confounding variables.
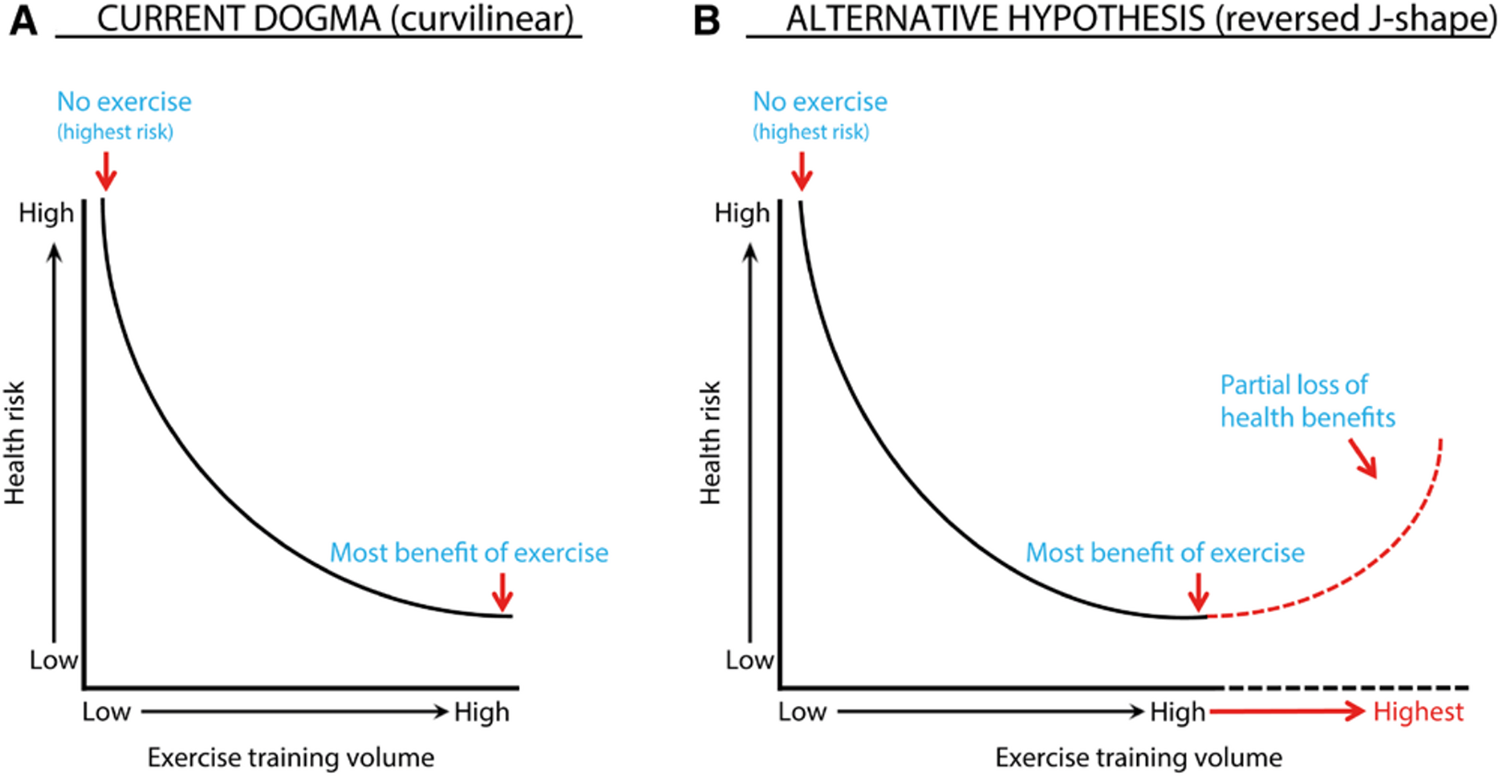
Across the included studies, most findings indicated that engaging in strenuous PA was either beneficial or neutral, with cardiovascular benefits levelling off at very high doses rather than continuing to increase. Two studies [23, 39] reported a U-shaped association, suggesting that strenuous PA was associated with a loss of cardioprotective benefit compared with more moderate doses. In both studies, the confidence intervals around these estimates were wide and not statistically significant, and the apparent patterns were difficult to interpret given the small number of participants engaging in strenuous PA, imprecise exposure classifications, and other methodological limitations identified in the risk of bias assessment. Overall, the broader evidence is more consistent with a plateauing of benefits, rather than a meaningful reversal of the protective effects of strenuous PA.
Classification of strenuous exercise intensity/measurement of PA
There are a variety of ways that strenuous PA is defined and reported. None of the studies in this review incorporated objective measures when assessing PA, instead opting for self-reported measures. Self-reported PA is commonly utilised in population research due to its low cost and simple assessment methods [50]. Despite its cost-effectiveness and ease of use, self-reported PA has been identified as having low correlations with objective measures, large variability between different assessment tools, as well as both over- and under-estimations of true behaviours [51, 52]. Therefore, none of the studies in this review received a low risk of bias grading for this domain. Most studies incorporated METs (except two studies [34, 36]) when calculating total PA levels but varied when estimating PA intensity.
Grouping vigorous activities with the same MET was common in the studies in this review. The majority of the included studies [23, 33, 35, 36, 38, 43] assigned a single MET value for all of the vigorous activities that were included in assessment tools. This approach increases the potential risk of bias as activities above or below the MET thresholds used are under- or over-estimating the true output for PA and potentially misclassifying individuals to a low, moderate or vigorous group. Four studies [37, 39, 41, 42] used precise estimations of METs when classifying an individual’s PA intensity. These studies utilised Compendiums of Physical Activities to obtain accurate estimates for PA intensity, which were developed to quantify energy costs (METs) associated with a large variety of activities, which ultimately increase the comparability of results across studies using self-reported PA [53].
Although the PA Compendiums are useful in estimating intensities, the variation between self-perceived PA intensity and the actual rate at which the heart is being exerted is a potential source of bias. This has been explored in a previous study comparing objective and subjective measures of PA intensity by Skatrud-Mickelson et al. [54]. This study found that regular exercisers (similar to those included in this review) underestimated exertion during PA and that the true intensity of exercise was in fact higher [54]. The use of self-perceived intensity data from self-reported measures ultimately increase the potential for bias to be present for the studies in this review, with variability in PA intensity potentially resulting in incorrect classification of individuals to moderate or vigorous PA categories and/or miscalculations for total PA energy expenditure [55]. Further issues begin to arise pertaining to the appropriate cut-off point for vigorous activity due to the varying MET estimates and calculations for total PA energy expenditure (weekly METs, MVPA mins etc.). As the studies in this review varied with the cut-off points used for intensities of PA (METs) and the different categories for total weekly energy expenditure (MVPA/TEE), the likelihood of one or more occurring prematurely increases the risk of individuals being misplaced into moderate sub-groups instead of their vigorous counterparts [56, 57]. These differences make comparisons of these studies more difficult and increase the chance for over- or underestimations of the true effect of vigorous PA on health.
Repeated PA measures/assessments
Repeated measurements help increase the reliability of exposure data, whilst also allowing researchers to investigate changes in behaviour over time [31, 58]. Janssen & Jollifee [36] was the only study in this review that measured PA behaviours more than once, with the authors assessing PA behaviours for the two weeks prior to examinations at both baseline and the initial three-year examination. This enabled the analysis of mortality risk relative to PA behaviours at both baseline and three-year follow-up, examining changes in PA behaviours. The inclusion of repeated PA assessments in these studies would have both strengthened the accuracy of PA data obtained from respondents, whilst also allowing the research groups to investigate whether changes in PA behaviour had an effect on outcomes and what levels of PA yielded the most protective benefits.
Outcome assessments
The vast majority of the studies in this review [23, 32, 34, 37, 39, 41, 42, 46] included mortality as a primary outcome variable. These studies ascertained the death status of individuals through death certificates, national databases, medical records and probabilistically matching. Although each of these studies used standardised methods to obtain the mortality status of individuals, there was some variation in cause of mortality. Of the studies that incorporated all-cause mortality as an outcome variable, only two [39, 41] provided additional analyses delving into disease specific mortality and received a low risk of bias rating, with the remaining studies [23, 32,33,34, 36, 42] incorporating deaths from any causes. The studies that included mortality from all causes only as an outcome variable received a moderate risk of bias grading, as their underlying causes of death were not strictly cardiovascular in nature or related to other relevant risk factors and could have been completely unrelated to cardiovascular health and PA. Two studies in this review incorporated outcome measures other than mortality. Maessen et al. [38] analysed the relationship between PA behaviours and CVD and the presence of cardiovascular risk factors (the presence of hypertension, hypercholesterolemia and/or type two diabetes), confirming an individual’s classification to either group against the medications they took. Aadahl et al. [35], took a similar approach but instead measured a range of biological variables during clinical examinations. Each of these two studies received a low risk of bias grading due to the standardised methods used to assess relevant risk factors for adverse cardiovascular events and mortality. The remaining studies [37, 43] included both mortality and a cardiovascular variable as outcome variables. Although the inclusion of cardiovascular biomarkers [37] and cardiovascular events [43] helped to provide a better understanding of the association between PA and cardiovascular outcomes using standard protocols, both studies included all-cause mortality. Consequently, these studies both received a moderate risk of bias grading as relevant cardiovascular data was included, but mortality was from all causes and not disease- or cardiovascular-specific.
Timeframe (follow-up)
As highlighted in the introduction, there are various clinical pathways through which PA can lead to a cardiovascular event, but a common pathway is that long-term excessive endurance exercise may induce pathologic structural remodelling of the heart and large arteries [22]. Therefore, a substantial timeframe is required to observe PA levels and cardiovascular/mortality outcomes. Two studies [35, 37] in this review were limited in their examination of the true effect of their exposure on their outcome(s) due to their cross-sectional components of their data collection, ultimately resulting in a high likelihood of bias [59]. For three of the cohort studies [34, 36, 39], the time for follow-up increased the potential for bias, as participants were followed over an average timeframe less than ten years. Six studies [23, 33, 40,41,42, 44] in this review had a timeframe for follow-up between ten and twenty years with a lower potential for bias. Two studies in this review [38, 43] had follow-ups that were longer than twenty years. Despite this, the study by Maessen et al. [38] has a high probability of bias as the timeframe for follow-up was based on recall data. Lifelong exercise patterns in this study were assessed by asking participants to recall their exercise habits across four life periods. Although participants were able to provide sufficient data, recall bias could be present and influence the accuracy of PA data provided. The timeframe (mean 23.4 ± 11.7 years) used by Joseph et al. [43] allows for the effects of high doses and intensities of PA to occur, and any associated adverse cardiovascular events to take place. This is the only study in this review that has received a low risk of bias grading. Greater timeframes to examine the effects of PA on cardiovascular/mortality outcomes are needed to reduce the potential for bias in the majority of the studies in this review.
Confounders/covariates
Incorporating relevant confounding factors increases confidence in establishing real relationships and contributes to the internal validity of the research. When examining the relationship between vigorous PA and cardiovascular risk factors, as well as mortality, there is a necessity to control for body weight, smoking status, dietary intake as well as blood pressure and blood cholesterol, as they are associated with adverse cardiovascular outcomes and mortality [4, 60]. In addition to these prominent risk factors, further adjustments need to be made with regard to sociodemographic variables (age, sex, race, education, marital status, residence, SES) and chronic disease status due to independent associations with overall health and wellbeing, cardiovascular events and mortality risk [61,62,63].
Overall, controlling for confounding in the statistical analyses varied for the fourteen studies in this review. All of the studies in this review allowed for potential confounders such as age and sex of respondents, which is standard practice in health research due to the independent effects of each variable on both general and cardiovascular-specific health [64, 65]. Age is a well-established cardiovascular risk factor, with older adults experiencing substantially higher rates of cardiovascular events and mortality than younger individuals due to age-related physiological changes and accumulation of risk factors over time [66]. Age may therefore act as an important effect modifier in the relationship between strenuous PA and cardiovascular outcomes; however, none of the included studies formally examined age-stratified effects or tested for interaction. Smoking status was incorporated into all studies excluding one [37], as it would have moderately reduced the total sample size for this study. Both level of education and marital status are commonly used as confounding variables, however, level of education was used in seven studies [23, 33, 34, 38, 39, 41, 43], whereas marital status was only present in three studies [33, 34, 41]. A variety of other sociodemographic variables were scarcely used across the fourteen studies in this review including race [36, 37], soc

Comments (0)