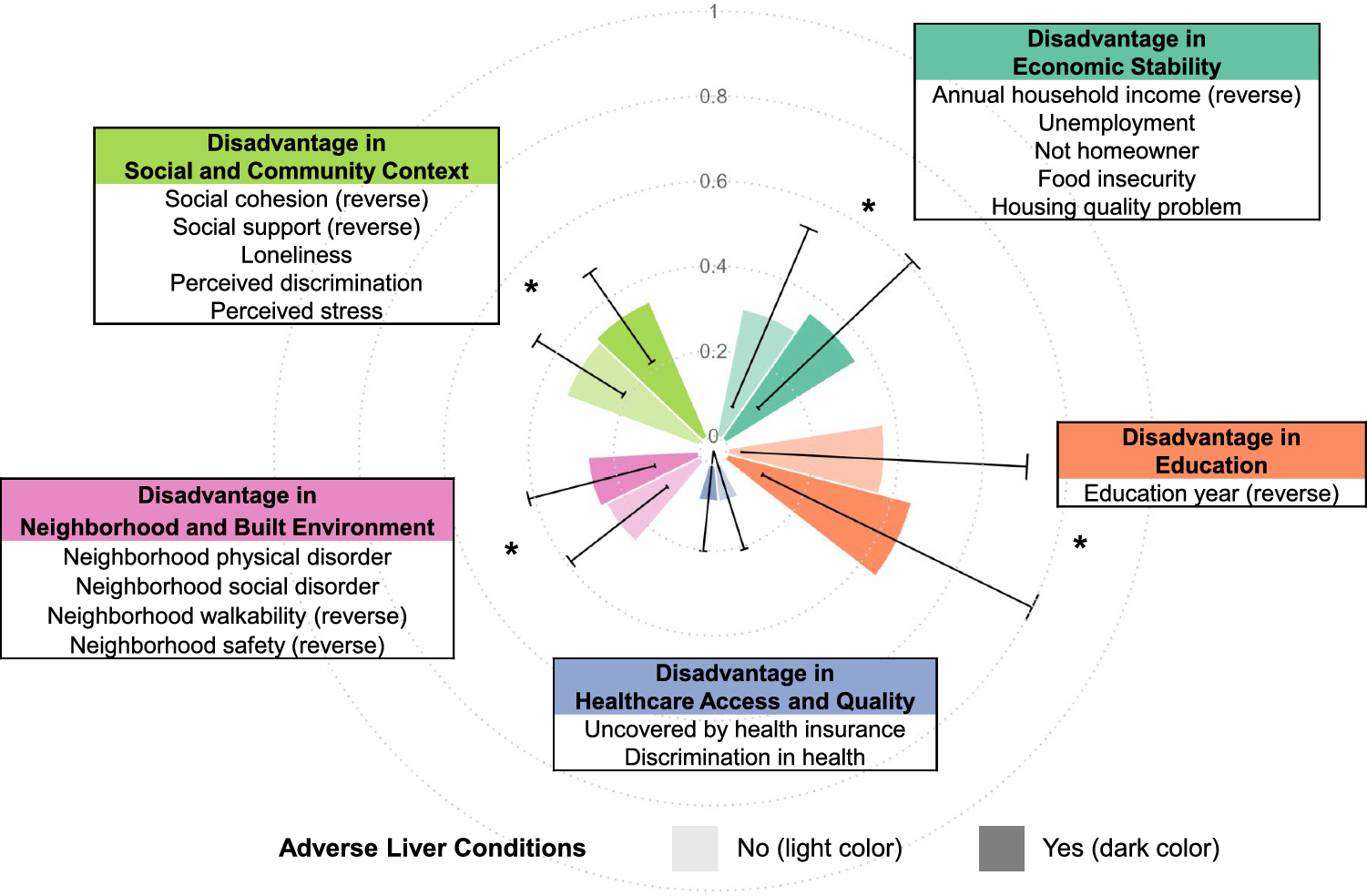
In this large-scale cross-sectional study, we proposed a systematically constructed score, SDDS, that captured all domains of disadvantage contributing to inequitable health outcomes. We found that disadvantage in structured SDOH, as assessed by individual domains, variables, and SDDS, was associated with poorer liver health. Disadvantage in economic stability, education, health care access and quality, neighborhood and built environment, and social and community context was independently associated with a higher likelihood of having total and individual adverse liver conditions. These associations remained robust after adjusting for key personal demographics and lifestyles such as age, sex, race, ethnicity, country of birth, marital status, smoking, alcohol drinking, obesity and T2DM. The associations remained consistent when excluding any missing data and using an alternative score with all five domains but fewer variables. The effect sizes illustrate that social disadvantage operates as a risk factor, comparable in magnitude to established metabolic and lifestyle factors. A 10% increase in the SDDS represents a meaningful shift in cumulative social disadvantage across multiple domains, and the corresponding increases in odds of adverse liver conditions underscore the clinical sensitivity of liver health to incremental social burden.
In context with previous literature
Our study, for the first time and in a large sample size, reported the significant, independent associations of each SDOH domain with prevalent adverse liver conditions. Results are in line with previous literature on the associations of key individual variables on liver diseases. For example, a key assessment of economic stability, food insecurity, was associated with liver fibrosis and an increased risk of advanced fibrosis and cirrhosis in a cross-sectional study of 3502 US adults in NHANES [19]. However, for other domains, their associations with the prevalence or incidence of liver diseases in the general population have not been well quantified. Studies that simultaneously evaluate multiple SDOH domains are sparse.
A few studies have examined social factors in individuals with liver disease. A study of 11,107 participants with chronic liver disease in Italy found that low educational level was associated with higher disease severity [20]. In the U.S. national cohort of Veterans Health Administration (VA), rural residents had a lower likelihood of accessing gastroenterology or hepatology specialty care compared to their urban counterparts [21]. However, the comparison of quality of care with disease incidence or prognosis was out of the scope of these studies. A recent retrospective cohort study found that disadvantage in neighborhood-level SDOH was associated with mortality, incidence of adverse liver conditions, and incident cardiovascular disease in 15,904 individuals with SLD [22]. However, the neighborhood SDOH was assessed by only the average income, education, and occupation status of households in the neighborhood. For the social and community context, a study on liver transplant recipients found that social support was positively correlated with self-management and hope [23]. Taking together the more comprehensive results from our study, we hope to raise awareness of SDOH for liver health.
A recent study using the All of Us dataset developed an SDOH score specifically for coronary heart disease (CHD), showing that all five domains were associated with the prevalence of CHD [24]. Compared to their data-driven approach using elastic net regression, our method is independent of specific disease events, more resilient to data bias and missing data, and may have potential for generalizability across different diseases and studies. We plan to evaluate the SDDS across other conditions within the All of Us cohort and in external studies.
Impact
Comprehensive individual-level data on SDOH are challenging to collect and may be prone to inaccuracies. We designed SDDS to be flexible and adaptable for use in diverse populations including study populations where data collection may be limited. For instance, if only one or two variables are available within a domain, these variables still should be able to effectively describe disadvantage status. By standardizing scores within the population, the SDDS is also adaptable to the heterogeneous distribution of data and the assessment tools used within each population. Compared to a few previous assessments of SDOH, our study captures wider domains and can examine their synergistic effects on health outcomes [25, 26]. Compared to other approaches to measuring SDOH using aggregate data, our methods individual-level variations [27,28,29]. Although future studies are warranted to validate this score and more data are needed to refine cutoff values, our conceptual approach to SDDS enables a standardized quantification and comparison of disadvantages, laying a foundation for consistent use in various settings. Because the SDDS provides a standardized, domain-based quantification of social disadvantage, it can be incorporated into screening. Clinically, the SDDS could be used with metabolic and lifestyle risk factors to flag patients whose social context places them at elevated risk for adverse liver outcomes. In public health practice, the SDDS can support population-level risk stratification, guide resource allocation, and inform upstream interventions that address modifiable social and structural drivers of liver disease.
Strengths and limitations
This study has several notable strengths. It is the first to employ a structured SDOH framework for liver conditions, using one of the largest sample sizes available (> 100,000) by leveraging a nationwide representative study. The use of validated questionnaires and scales ensures the robustness and reliability of the data collected. Furthermore, our study includes diverse participants and considers groups underrepresented in biomedical research, such as diverse racial and ethnic groups. Importantly, we validated the SDDS against liver conditions, a critical and leading health concern, demonstrating the practical relevance and impact of this score on public health.
Limitations should be noted. First, although the All of Us reflects the diversity of the U.S., it cannot be described as a representative sample [13]. The results may not generalize to populations with different SDOH. Second, the All of Us program does not focus on any particular set of diseases, enabling the study of various diseases and health status but meanwhile limits the detailed, specific information on disease of interest, in this case, the diseases of the liver. Third, the potential underdiagnosis of liver disease by EHR highlights the need for future studies replicating our approaches. Despite this, our findings may still hold scientific validity, as the associations observed between social disadvantage and liver conditions are consistent with known risk patterns. Additionally, underdiagnosis could bias the results towards the null, suggesting that the true associations may be even stronger. Last, longitudinal follow-up studies are warranted to address the impact of SDOH on chronic, adverse liver conditions. Such studies would allow for causal inference, providing insights into how social disadvantage influences liver disease development and progression over time. They could also identify critical windows for intervention and inform strategies to mitigate the burden of liver disease in vulnerable populations.
To conclude, we developed the Social Determinants Disadvantage Score (SDDS) as a comprehensive tool for assessing social disadvantage in future studies. By validating this score against liver conditions, we addressed a significant knowledge gap in understanding the associations between SDOH and liver health. Our findings reveal clear and dose–response associations between higher SDDS and higher risk of adverse liver conditions, highlighting the importance of social factors in liver health and providing a strong foundation for future research and potential interventions.

Comments (0)