Study design and population
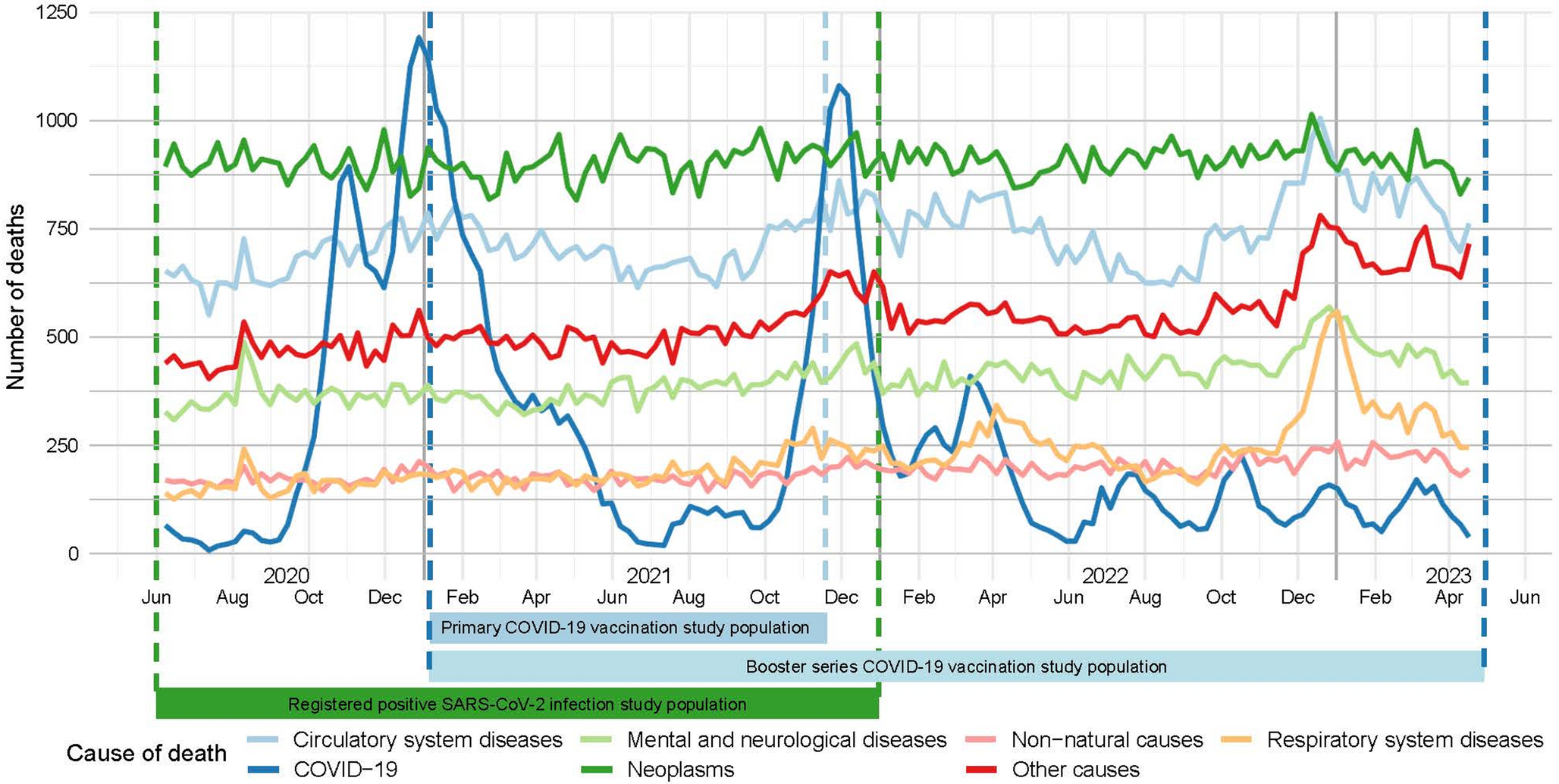
We performed an retrospective study using a SCCS design and record linkage approach in the general Dutch population. The study included Dutch inhabitants registered in the General population Personal Records Database (BPR) governed by Statistics Netherlands (CBS). For the analysis on the effect of primary COVID-19 vaccination, all subjects who died between January 6, 2021, the first day of vaccine administration in the Netherlands, and November 18, 2021, the start of the booster campaign were included. For the analysis on the effect of booster vaccinations, we additionally included subjects who died until April 30, 2023, the last recorded date in the mortality database at time of the study. For the analysis on the effect of a registered positive SARS-CoV-2 infection, inhabitants who died between June 1, 2020 and December 31, 2021 were included, during the period when tests were registered.
All data sources were linked by an unique pseudonymized identifier. CBS is bound by the European General Data Protection Regulation. In addition, CBS adheres to the privacy stipulations in the Statistics Netherlands Act, the European Statistics Code of Practice, and its own Code of conduct. Informed consent is not feasible for this study since all research data is pseudonymized. This study falls within the exceptions mentioned in Sect. 5 of the code of conduct for medical research. This study was conducted according to ‘gedragscode gezondheidsonderzoek’, the principles of the Declaration of Helsinki (World Medical Association, 2013) and in accordance with the EU GDPR (General Data Protection Regulation). This study does not fall under the scope of the Dutch Medical Research Involving Human Subjects Act (WMO). It therefore does not require approval from an accredited medical ethics committee in the Netherlands. However, in the UMC Utrecht, an independent quality check has been carried out to ensure compliance with legislation and regulations (regarding Informed Consent procedure, data management, privacy aspects and legal aspects).
Outcomes
The primary outcome of this study was death from any cause. As a secondary outcome, non-COVID-19 related death was examined. Notification of the cause, time, and location of death is mandatory under Dutch law. The cause of death is initially determined by the attending physician, who completes a medical death certificate indicating the sequence of events leading to death and any underlying condition. Death certificates are processed and coded by CBS into The National Cause of Death Registry (1995–2023). From this registry, the date and cause of death were extracted. The event or disease that initiated the process of events that led to death is registered according to the International Statistical Classifications of Diseases and Related Health Problems, 10th revision (ICD-10) of the World Health Organization (WHO) [23]. COVID-19 deaths were defined based on the ICD-10 codes for proven (U07.1) or suspected COVID-19 (not tested or virus not identified; U07.2). The WHO defines a death due to COVID-19 for surveillance purposes as a death resulting from a clinically compatible illness in a probable or confirmed COVID-19 case, unless there is a clear alternative cause of death, and without a period of complete recovery from COVID-19 between illness and death [24]. Non-COVID-19 related causes of death were grouped into six umbrella categories as used by Statistics Netherlands including neoplasms; circulatory system; respiratory system; mental, behavioral, and nervous system; external (non-natural) causes; and other natural causes [2].
COVID-19 vaccination
COVID-19 vaccination data was obtained from the COVID-vaccinatie Informatie- en Monitoringssysteem (CIMS) (2020–2023) governed by the National Institute for Public Health and the Environment (RIVM). CIMS contains information on individuals who have consented to be registered in the vaccine registry. The COVID-19 vaccination campaign for the primary series started on 6 January 2021 in the Netherlands according to priority groups. The booster series started on 18 November 2021. Vaccination uptake was 87.4% among people aged 12 and over at the end of 2021 [25]. Permission for registering vaccine administrations in the database was granted by 93% of participants for the primary series, 95% for the booster series, and 99% for the repeated dose. From this registry, the date of vaccination, vaccine batch, type of vaccination, vaccine dose, and administrator was extracted. The type of vaccine was categorized as mRNA (Pfizer/BioNTech, and Moderna) and non-mRNA or unknown (AstraZeneca, Janssen, Novavax, Valneva, Sanofi Pasteur, HIPRA, or vaccine type unknown). The primary series was considered completed and effective 14 days after a subject received two or three (only indicated for immunocompromised individuals) primary vaccinations with either Spikevax® (Moderna), Comirnaty® (Pfizer-BioNTech), Nuvaxovid® (Novavax), or Vaxzevria® (AstraZeneca), or as a single dose of the Janssen COVID-19 Vaccine, as per national guidelines at the time [26]. Alternatively, a completed primary series could be defined as a single vaccine dose of the Moderna, Pfizer, Novavax or AstraZeneca vaccine in subjects with a documented prior SARS-Cov2 infection. SARS-CoV-2 infection.
Information about reported SARS-CoV-2 infections to the Dutch municipal health services were obtained from a database governed by the municipal health services [HPZone Lite van de gemeentelijke gezondheidsdiensten, GGDCOVID19BM] (2020–2021). At the time of the study-period, COVID-19 was a notifiable disease in the Netherlands meaning that all positive SARS-CoV-2 infections had to be reported to a municipal health service. From this registry, the registration date of a SARS-CoV-2 infection and type of SARS-CoV-2 test were extracted. A positive reporting within 90 days of a previous positive report was assumed to belong to the previous SARS-CoV-2 infection episode and excluded [27]. At the start of 2021, the SARS-CoV-2 wildtype dominated in the Netherlands, the Alpha variant dominated in Spring 2021, and Delta dominated from June 2021 onwards until Omicron BA.1 replaced Delta at the end of the year.
Covariates
Sex and age group (10–20 years band) were extracted from the population registry governed by Statistics Netherlands. Comorbidities before the date of first vaccination or SARS-CoV-2 infection were defined on the basis of hospital admission information and were extracted from the Dutch Hospital Discharge Registry (DHDR) governed by the Dutch Hospital Data (DHD) foundation. The hospital admission and discharge data, institutions number (pseudonymized), admission number (pseudonymized), and diagnoses recorded as ICD-10 code (as of 2014) and ICD-9 code (1995–2013) were extracted from this database [23, 28]. The comorbidities were specified according to the ECDC core protocol for COVID-19 vaccine effectiveness studies including asthma, immunodeficiency (including HIV infection) and organ transplant, cancer, diabetes mellitus, heart disease (excluding hypertension), hypertension, lung disease (excluding asthma), obesity, anemia, asplenia, chronic liver disease, neuromuscular disorders, renal diseases, dementia, stroke, rheumatologic diseases and tuberculosis [29].
Statistical analysis
Data linkage and statistical analyses were conducted using R version 4.4.4.
A modified SCCS method was used to estimate the incidence rate ratio (IRR) and 95% confidence intervals (CI) of death in a predefined risk interval compared to a predefined control interval [16]. This modification is designed to handle multiple event-dependent exposures, such as COVID-19 vaccine administrations, in relation to death as the event of interest. With death as the event of interest, the key assumptions of a standard SCCS are violated, as death precludes subsequent exposures and observation periods. This modified SCCS compares the risk of death during a predefined risk period following exposure to a reference period, defined as all observation time during which subsequent exposures could have occurred. This makes the end of the observation period independent of events. The model parameters are estimated by iteratively reweighting observations to align with a counterfactual scenario in which no exposures can occur after death, ensuring that death does not censor exposures, as there are no exposures in this counterfactual scenario.
The SCCS models were fitted using a conditional Poisson regression model using a pseudo-likelihood method on a person-week level dataset [16, 30, 31]. The IRRs for deaths in the risk interval relative to the control interval were estimated. The 95% CI for the parameters were obtained using the sandwich estimator in which the inverse Jacobian matrix surrounds the observed covariance matrix of the estimating functions [32, 33]. The length of each week in days was included as an offset in the model, as some weeks are not complete (such as if a vaccination occurs part way through a week). The risk interval was defined as day 1 to 21 days following COVID-19 vaccine administration, excluding day 0 from analyses, or as day 0 to 21 following a registered positive SARS-CoV-2 infection. We examined the first three weeks combined, and for each of the three weeks individually. The control interval was defined as all the following weeks to the end of the study. For vaccination, the risk weeks were further categorised by dose or considered for all doses combined. Due to the within-person comparison, time-invariant confounding, such as sociodemographic factors, comorbidities and health-seeking behaviour, is automatically controlled for. To account for time trends in mortality incidence due to seasonality and fluctuating SARS-Cov-2 infection rates, calendar time in two-week intervals was included as a covariate in the analysis. This time-trend adjustment is independent of vaccination status and thus included individuals who died with no registered vaccine administration or infection to avoid bias [16].
Subgroup analyses
Analyses were stratified by sex, age group at start of the observation period (12–29, 30–39, 40–49, 50–59, 60–69, 70–79, 80–89, ≥ 90) and presence of comorbidities (none, one, multiple). The subgroup aged < 12 was not analysed seperately to comply with privacy regulations of Statistics Netherlands. Analyses for the primary series were additionally stratified for vaccine type (mRNA or non-mRNA/unknown), and a prior registered positive SARS-CoV-2 infection before vaccination (yes/no). The analyses of each vaccine type included all individuals who received at least one dose of the vaccine type of interest. The doses were renumbered to correspond to the first, second, and third dose of the vaccine type of interest, while doses of other vaccine types were excluded by setting them as missing. Analyses for registered positive SARS-CoV-2 infection were additionally stratified by vaccination status at time of registration. ‘Sensitivity analyses.
Multiple sensitivity analyses were performed to assess robustness of findings or to test relevant secondary hypothesis. First, individuals with a positive SARS-CoV-2 infection in the 8 weeks before vaccination or during the exposure period were excluded. Second, calendar time adjustment was done using a restricted cubic spline to test whether this was a more realistic representation of confounding by calendar time effects. Third, we repeated the analysis without adjustment for calendar time, to evaluate its impact. Third, we fitted a model with 12 weekly risk intervals to estimate week-specific effects, and separate models with cumulative risk periods up to 12 weeks to assess sensitivity to the specification of the risk period. Fourth, analyses were stratified according to administrator (municipal health services, general practitioner, or other) to account for possible difference in patient populations and to identify potential inconsistencies in data registration. Lastly, a, 2-, 4-, 7- and 14-day induction interval before the registration date of positive SARS-CoV-2 was applied (excluding observation time immediately preceding the index date) to account for potential delays in test registration.

Comments (0)