
Remember me

Among 1341 screened patients with AB group pneumonia, 106 met the inclusion criteria (HD: 46; SD: 60) (Table 1). The cohort comprised 77 males (72.6%) and 29 females (27.4%). Male patients were numerically more frequent in both the HD (65.2%) and SD (78.3%) groups, though this difference was not statistically significant (p = 0.187). Baseline APACHE II scores were similar between groups (HD: 26 vs. SD: 24; p = 0.385), but Charlson comorbidity index was lower in the HD group (6 vs. 7; p = 0.027). Chronic kidney disease and type 2 diabetes mellitus were more frequent in the HD group (p = 0.029 and 0.046, respectively), while thoracic drain placement was more common in the SD group (p = 0.006). Other baseline comorbidities and rates of invasive procedures were comparable. Although 28-day mortality did not differ significantly (13% vs. 18.3%, p = 0.594), the HD group was associated with a significantly lower in-hospital mortality rate compared to the SD group (28.3% vs. 48.3%, p = 0.046). Among survivors, patients treated with HD minocycline had numerically shorter ICU stays compared with the SD group (median 12 vs. 23 days, p = 0.745) and shorter duration of mechanical ventilation (median 19 vs. 29 days, p = 0.248). Although these differences did not reach statistical significance, the trends were consistent with a potential benefit of HD therapy.
Table 1 Clinical characteristics among patients with Acinetobacter baumannii group pneumonia classified according to minocycline treatment doseRisk Factors for MortalityThe risk factors for in-hospital mortality were further analyzed as listed in Table 2. There were 42 (39.6%) patients died during the hospitalization. Among the 42 non-survivors, the causes of death were as follows: uncontrolled infection (n = 36, 85.7%), advanced cancer (n = 4, 9.5%), cardiogenic shock (n = 1, 2.4%), and cerebral hemorrhage (n = 1, 2.4%). There was no significant difference in mortality between the sexes (male, 31/77 [40.2%]; female, 11/29 [37.9%]). Higher APACHE II scores (median 28 vs. 21, p = 0.001), chronic kidney disease (71.4% vs. 51.6%, p = 0.046), and chemotherapy (28.6% vs. 10.9%, p = 0.036) were significantly associated with in-hospital mortality. Survivors were more likely to have received HD minocycline (51.6% vs. 31.0%, p = 0.046), while appropriate antimicrobial therapy rates did not differ between groups.
Table 2 Clinical characteristics of patients with Acinetobacter baumannii group pneumonia who survived or died in hospitalMultivariate analysis showed that chronic kidney disease (adjusted OR, 9.019; 95% CI, 1.844–44.177; p = 0.007) and chemotherapy (adjusted OR, 5.693; 95% CI, 1.212–26.737; p = 0.028) were independent predictors of in-hospital mortality (Table 3). HD minocycline was the only protective factor for in-hospital mortality (adjusted OR, 0.183; 95% CI, 0.050–0.680; p = 0.011). A PS of receiving HD minocycline was calculated. Variables with p value < 0.1 for both the treatment and outcome groups (Tables 1 and 2) were included in the PS (Supplementary Table S1). The balance of PS covariates between the two treatment groups, both before and after PS weighting, is presented in Supplementary Table S2. Histograms of propensity score demonstrated substantial overlap between patients receiving SD and HD minocycline (Supplementary Figure S1). After IPTW using ATT frameworks, improved covariate balance was achieved. SMDs for key baseline covariates were markedly reduced after IPTW using the ATT frameworks (Supplementary Figure S2). Under the ATT framework, HD therapy was significantly protective (weighted OR: 0.307; 95% CI 0.111–0.844).
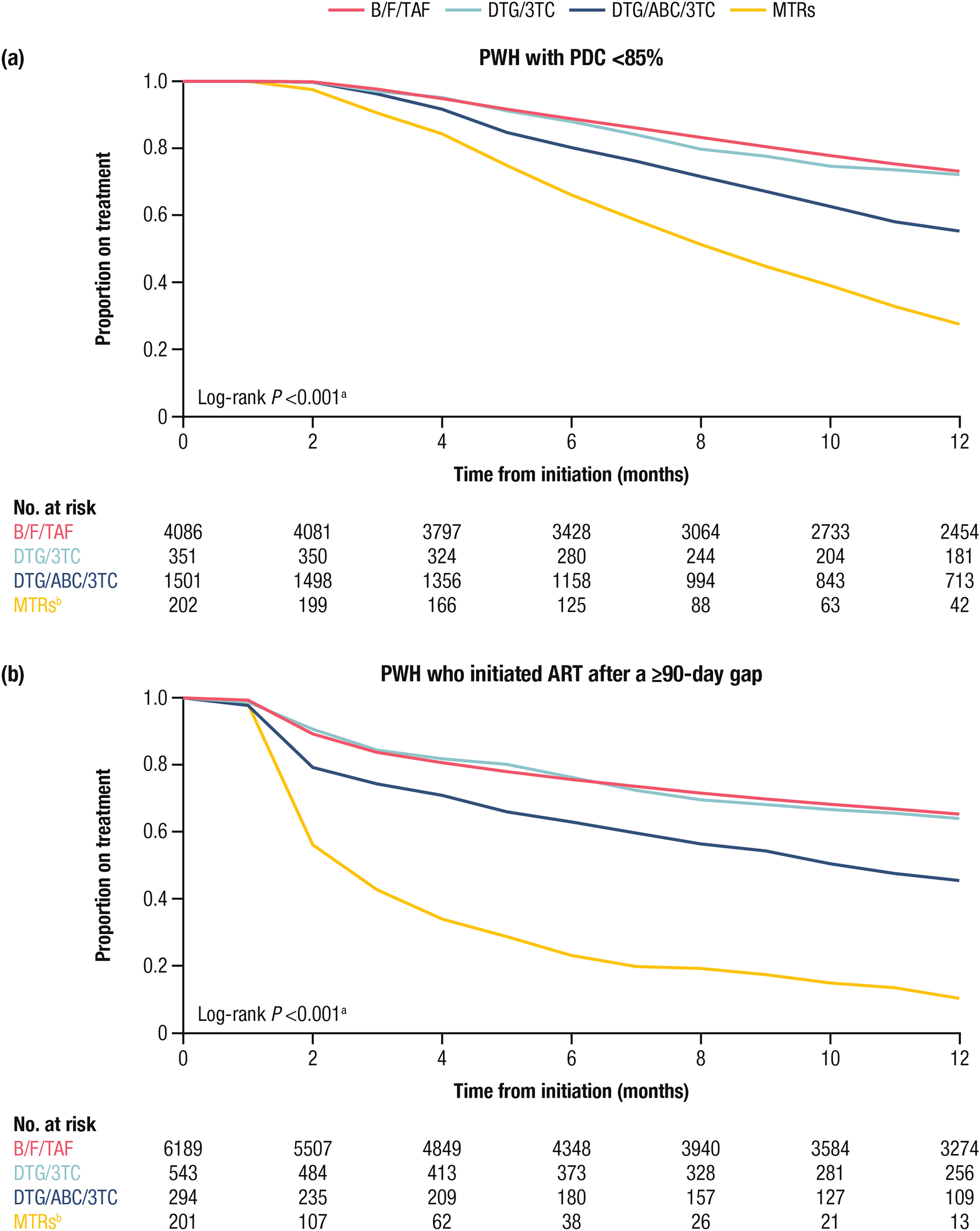
Table 3 Multivariable and Inverse probability of treatment weighting-adjusted logistic regression analysis of factors associated with in-hospital mortalityKaplan–Meier Survival AnalysisKaplan–Meier survival curves showed no significant difference in 28-day survival between the HD and SD groups (log-rank test, p = 0.253), suggesting HD minocycline improves in-hospital but not short-term survival. For long-term outcomes, Kaplan–Meier survival curves up to 150 days after pneumonia onset demonstrated a significant survival benefit with HD therapy compared with SD therapy (log-rank test, p = 0.028). The survival curves separated gradually over time without an early divergence and remained apart thereafter (Fig. 1).
Fig. 1
Kaplan–Meier survival curves at 150 days after Acinetobacter baumannii group pneumonia onset for patients receiving high-dose or standard-dose minocycline therapy. HD vs. SD, log-rank test, P = 0.028. HD high-dose minocycline, SD standard-dose minocycline
Minocycline MIC Profiles and Outcomes Stratified by MIC and Minocycline DoseBecause of institutional practice variability, minocycline MIC testing was only performed at TVGH since mid-2023. Among the 57 AB group isolates collected from this center, MIC data were available for 28 strains. The MIC distribution was as follows: ≤ 1 µg/ml (n = 7, 25.0%), 2 µg/ml (n = 4, 14.3%), 4 µg/ml (n = 9, 32.1%), 8 µg/ml (n = 6, 21.4%), and ≥ 16 µg/ml (n = 2, 7.1%). The MIC50 and MIC90 were 4 µg/ml and 8 µg/ml, respectively. Among the 28 isolates with available MIC data, most were A. baumannii (n = 24). The MIC distribution within this group was broad (MIC ≤ 1, n = 4; MIC = 2, n = 4; MIC = 4, n = 9; MIC = 8, n = 5; MIC ≥ 16, n = 2). The remaining isolates included A. nosocomialis (n = 1, MIC ≤ 1), A. pittii (n = 1, MIC ≤ 1), and A. seifertii (n = 2; MIC ≤ 1 and MIC = 8). Due to the small number of non-baumannii isolates, no statistically or clinically meaningful correlation between subspecies and MIC distribution could be established.
Based on CLSI 2024 breakpoint (susceptible ≤ 4 µg/ml) and PK/PD breakpoint (susceptible ≤ 1 µg/ml) [12], 28.6% and 75.0% exhibited elevated MICs above the susceptibility threshold, respectively. Among 28 patients with available MIC-confirmed isolates, outcome patterns varied by minocycline dose and susceptibility level (Fig. 2, Supplementary Table S3, Supplementary Figure S3). In patients infected with isolates exhibiting MICs ≤ 4 µg/ml (n = 20), those receiving HD minocycline (n = 14) had lower in-hospital mortality (4/14, 28.6%) compared to those receiving SD therapy (n = 6; 4/6, 66.7%). The difference did not reach statistical significance (p = 0.161), likely due to limited sample size. Among patients with MICs ≥ 8 µg/ml (n = 8), in-hospital mortality remained lower with HD therapy (2/7, 28.6%) versus SD therapy (1/1, 100%). Using the PK/PD breakpoint of MIC = 1 µg/ml, patients with MIC ≤ 1 who received HD minocycline experienced no in-hospital deaths (0/3), whereas those treated with SD therapy had a 75% mortality rate (3/4). Although this difference was clinically meaningful, it did not reach statistical significance (p = 0.143). In the MIC ≥ 2 group, in-hospital mortality was 33.3% (6/18) in the HD group and 66.7% (2/3) in the SD group (p = 0.531). These findings suggest a potential benefit of HD therapy across MIC strata, but further studies are warranted due to limited sample size.
Fig. 2
In-hospital mortality by minocycline dose under two minimum inhibitory concentration (MIC) classification schemes in patients with Acinetobacter baumannii group pneumonia. Each pair of bars compares high-dose (HD; 200 mg IV q12h) and standard-dose (SD; 100 mg IV q12h) minocycline for in-hospital mortality within strata defined by two different breakpoints: (1) Pharmacokinetic/pharmacodynamic (PK/PD)-based breakpoints (≤ 1 µg/ml vs ≥ 2 µg/ml) and (2) 2024 Clinical and Laboratory Standards Institute (CLSI) breakpoints (≤ 4 µg/ml vs ≥ 8 µg/ml). Data are limited to 28 patients with available MIC-confirmed isolates. Across both classification methods, HD therapy was consistently associated with a lower mortality rate than SD therapy, although differences did not reach statistical significance due to limited sample size
These findings also highlight a key distinction between the CLSI 2024 breakpoint (≤ 4 µg/ml) and the PK/PD-derived breakpoint (≤ 1 µg/ml). Specifically, in the HD group, only the PK/PD breakpoint was able to differentiate survival outcomes, whereas the CLSI 2024 breakpoint failed to discriminate in-hospital mortality. In contrast, among patients receiving SD minocycline, neither breakpoint effectively differentiated mortality risk.
Microbiological Profiles and TherapyIn terms of microbiology, significantly more patients in the HD group were infected with A. baumannii (82.6% vs. 51.7%, p = 0.001). The prevalence of carbapenem-resistant (CR) and MDR isolates did not differ significantly between the groups. Combination regimens, including antipseudomonal cephalosporins, piperacillin-tazobactam, carbapenems, and colistin, were used in both groups. HD minocycline was more frequently combined with piperacillin-tazobactam (26.1% vs. 6.7%, p = 0.012). The rate of appropriate antimicrobial therapy was similar between groups (30.4% vs. 31.7%, p = 1.000).
To demonstrate the impact of antimicrobial regimen on in-hospital mortality, patients were stratified by their antimicrobial regimens (Table 4). Minocycline plus antipseudomonal cephalosporins (18.9%) was the most common regimen, followed by minocycline plus carbapenems (17.9%). No significant differences in in-hospital mortality were observed among HD recipients across different combination therapies.
Table 4 Antimicrobial regimens for the treatment of Acinetobacter baumannii group pneumoniaYear-by-Year Minocycline MIC SurveillanceA year-specific analysis of A. baumannii group isolates at TVGH revealed temporal trends in minocycline susceptibility. MIC testing for minocycline began at Taipei Veterans General Hospital in mid-2023. Despite this difference in sampling window, the MIC distribution patterns were comparable between the 2 years. In 2023, 325 isolates underwent MIC testing: 75 (23.1%) had MIC ≤ 1 µg/ml, 73 (22.5%) had MIC of 2 µg/ml, 82 (25.2%) had MIC of 4 µg/ml, 53 (16.3%) had MIC of 8 µg/ml, and 42 (12.9%) had MIC ≥ 16 µg/ml. The cumulative proportion of isolates with MIC > 1 and > 4 µg/ml was 77.5% and 29.2%, respectively. In comparison, 2024 surveillance data (n = 330) showed a similar MIC50 and MIC90 (4 and 8 µg/ml, respectively), with the distribution as follows: ≤ 1 µg/ml (n = 104, 31.5%), 2 µg/ml (n = 61, 18.5%), 4 µg/ml (n = 72, 21.8%), 8 µg/ml (n = 70, 21.2%), and ≥ 16 µg/ml (n = 23, 7.0%). The proportion of isolates with MIC > 1 and > 4 µg/ml was 68.5% and 28.2%, respectively. These surveillance data suggest a persistently high proportion (~ 28–29%) of A. baumannii isolates with high-level minocycline resistance.
Comments (0)