Study Design and Population
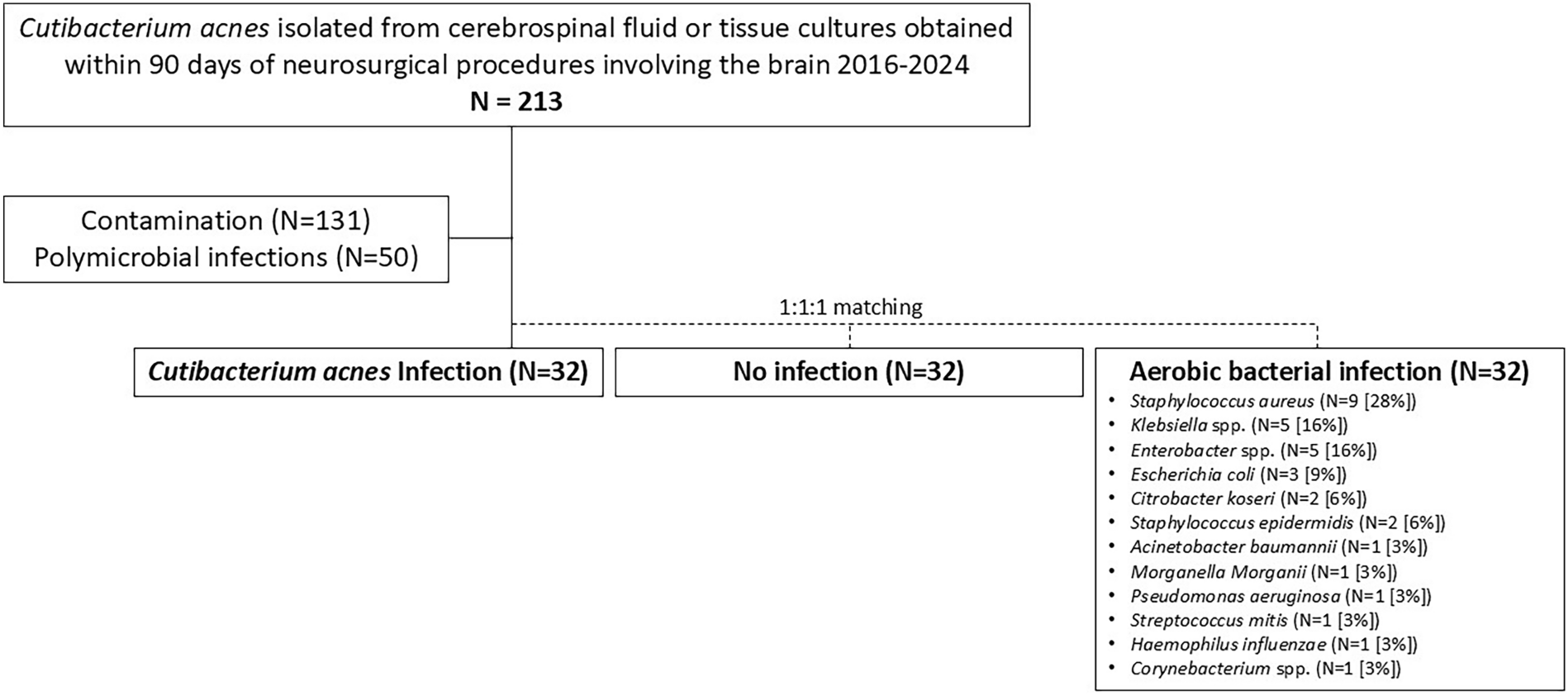
This was a single-center, observational, case–case–control study [10] assessing both clinical correlations for infection and predictors of poorer outcomes of CNS infections caused by C. acnes at Sheba Medical Center (SMC), between April 2016 and April 2024. SMC is a ~1600 bed, university-affiliated tertiary healthcare center, that provides neurosurgical care to patients referred from other hospitals in the region. The Neurosurgery Department at SMC performs approximately 2000 surgical procedures per year, and includes 40 beds, comprising 10 neurosurgical ICU beds and 4 step-down beds. We included adult patients (age > 18 years) who underwent a cranial neurosurgical procedure (see definitions), from whom C. acnes was isolated from either the CSF, a tissue sample collected during a repeated procedure, or from a percutaneously drained empyema or abscess within 90 days following the index procedure. Their medical records were reviewed and classified as either a true infection or contamination resulting from dermal colonization (see definitions). Isolates deemed to merely reflect contamination were excluded, whereas those classified as true infections were included as cases (cases I), comprising the basic cohort of the current study. We then randomly sampled individuals who underwent cranial neurosurgery and either developed abIs (cases II) or did not develop infection (controls) during the 90-day period following the index procedure. Cases II and controls were matched to the cases I (1:1:1) by year of procedure (± 3 years), age at time of procedure (± 5 years), and type of procedure (major or minor, see definitions below). Cases II and controls were randomly sampled through a computerized algorithm programmed using structured query language (SQL).
Ethical Approval
The institutional review board at Sheba Medical Center prospectively approved the study protocol (IRB approval reference number SMC-0162-23). An exemption from informed consent was granted owing to the retrospective design. All methods were performed in accordance with the relevant guidelines and regulations.
Exclusion Criteria
Children (aged < 18 years)
Polymicrobial infections, defined as the isolation of > two different bacterial species from relevant medium within a 14-day interval
Isolations defined as contamination
Study Procedures
The study included two phases (Supplementary Fig. S1), aimed at addressing different research questions:
1.
Phase I: assessment of clinical correlates for postneurosurgical infection, particularly those unique for CaIs. In this phase, we treated the study groups as the dependent variable, and demographics, medical background, and characteristics of the index procedure as independent variables. Accordingly, we compared cases I versus controls and cases II versus controls.
2.
Phase II: assessment of infection manifestations and predictors of poorer outcomes. In this phase, we included only individuals diagnosed with postcranial neurosurgical infections (cases I and cases II). These two groups, along with background characteristics, infection presentation, and management were treated as independent variables. The primary outcome was clinical cure at 90 days, defined as a composite of all the following criteria: 1. no death; 2. resolution of fever; 3. improvement in the Glasgow Coma Scale (GCS) [11]. Sensitivity analyses were carried out by varying the outcome assessment timeframe to 7 and 180 days.
Laboratory Methods
Cerebrospinal fluid (CSF) and tissue specimens were processed in the Clinical Microbiology Laboratory (ISO 15129 accredited) located on campus, according to standard laboratory protocols. For isolation of anaerobes, samples were inoculated onto appropriate anaerobic culture media based on specimen type, and incubated in anaerobic jars under strict anaerobic conditions, or inoculated into thioglycolate broth, both incubated at 37 °C. In cases where turbidity developed in the thioglycolate medium, subculture onto solid anaerobic media was performed under the same temperature and anaerobic conditions. Throughout the study period, all aerobic and anaerobic microorganisms were identified using matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS; Bruker Daltonics, Germany). Antimicrobial susceptibility testing was performed according to the Clinical and Laboratory Standards Institute (CLSI) breakpoints relevant to the performance date.
Data Collection
We retrieved individuals patient data from medical charts, using the MDClone ADAMS platform (mdclone.com), including the following information: demographics: age at time of the index procedure, gender, and type of community residence (home, elderly home, long-term healthcare facility, or another hospital); baseline characteristics: smoking status (current, past, or never), basic physical capacity (completely able, limited in some activities, requires assistance in activities of daily living, or bedridden); comorbidities: Charlson comorbidity index [12] and immunosuppression (as defined in the supplementary material); surgical procedure details: type and indication, urgency status: elective versus urgent or emergent (per National Healthcare Safety Network [NHSN] definitions [13]), American Society of Anesthesiologists (ASA) physical status classification system [14], functional capacity, and GCS immediately before the procedure, shift during which the surgery was performed (morning, evening, or night), duration of surgery, perioperative antibiotic prophylaxis regimen, duration of postprocedural mechanical ventilation, type of drainage inserted, duration of drainage, presence and duration of a central venous catheter, ICU admission and duration; length of stay following the procedure, discharge status (to original accommodation, rehabilitation facility, another hospital, or deceased), GCS and functional capacity at discharge; infection presentation: signs and symptoms, blood parameters, need for reoperation, length of rehospitalization, antimicrobial resistance of the isolated bacteria (for aerobic infections); duration of antibiotic treatment; outcomes: repeated cultures, presence of fever and GCS at 7, 90, 180 days, and date of death.
Definitions
The index procedure was defined as a neurosurgery involving the brain, performed for an indication other than infection source control. In cases where multiple procedures were performed prior to the infection, the most recent procedure was considered the index procedure. The procedure was considered cranial neurosurgery if it included skull penetration. Procedures were identified using ICD-9 codes and categorized as either major (craniotomy, craniectomy, or cranioplasty) or minor (insertion or removal of ventricular drain, shunt, or parenchymal leads) (Supplementary Table S1).
C. acnes contamination was defined as the isolation of C. acnes in a patient who had not received antibiotics within a 14-day window surrounding the isolation, or when antibiotics had been prescribed for an unrelated infectious syndrome (e.g., pneumonia).
Postcranial neurosurgery infections were defined according to a modification of the surgical site infection criteria outlined in the NHSN guidance [13], and included infections occurring within the 90-day surveillance period following the index procedure. Given the potential for C. acnes to represent mere contamination, we included only cases with isolates from CSF or surgical samples. Accordingly, all included infections met the NHSN criteria for organ/space surgical site infections. We further classified infections into the following three categories: meningitis (positive CSF culture without associated parenchymal, subdural, and epidural abscesses); parenchymal abscesses; and empyemas. The latter classified as either epidural or subdural. Subdural empyemas contiguous with the epidural space were classified under subdural.
Statistical Methods
We compared the study groups implementing bivariate and multivariable conditional logistic regression models. Independent variables were selected for inclusion in the multivariable models on the basis of the results of the bivariate analysis (p < 0.10) and prior knowledge. Correlations between independent variables were assessed using Spearman’s rank correlation coefficient, and variables with high correlation (ρ > 0.5) were evaluated in separate models. Matched odds ratios (ORs) and 95% confidence intervals (CIs) were obtained from the conditional logistic regression models.
We included demographic data, baseline characteristics, comorbidities, and information related to the index procedures in the assessment of clinical correlates for infections. The two case groups, CaIs (cases I) and abIs (cases II), were analyzed separately, each compared with the control group. By directly comparing the models, we identified the clinical correlates specifically associated with CaIs.
To analyze clinical presentation, we compared the two case groups (cases I and cases II) to identify factors distinguishing CaIs from abIs. The analysis adjusted for potential interfering factors and included baseline characteristics, clinical syndrome, and laboratory parameters to identify clinical correlates of CaIs presentation. Outcomes were analyzed by comparing the proportion of patients who achieved clinical cure at the predefined time points. This allowed us to assess the impact of infection by either bacterial group (CaIs and abIs) on clinical outcome, while adjusting for baseline characteristics, clinical presentation, and management.
For all analyses, p < 0.05 was considered statistically significant. Data analysis was conducted IBM SPSS version 28 (Armonk, NY, USA).


Comments (0)