
Remember me
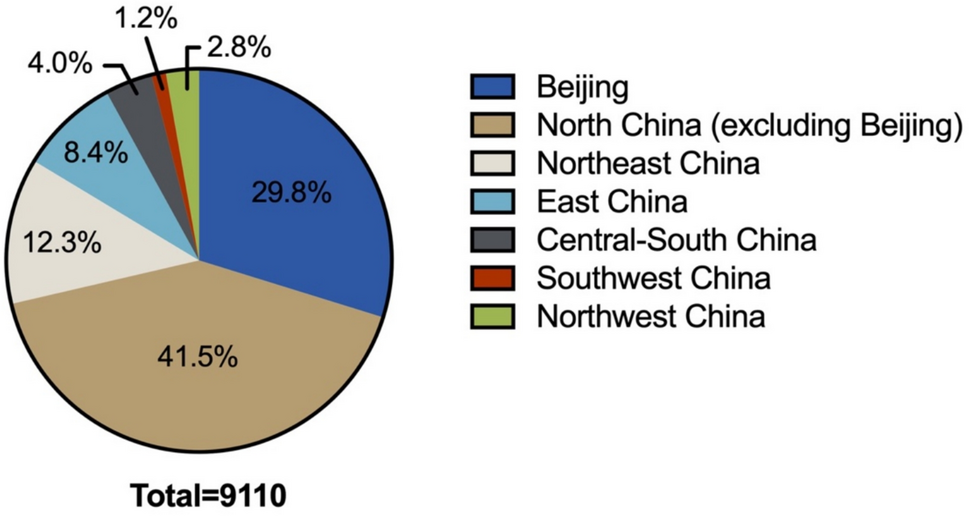


Within the cohort of 9,110 patients included in this study, the median age was determined to be 55 years, with a marked predominance of male participants. The distribution of tumor locations across both kidneys was found to be relatively equitable, and the majority of cases were classified as solitary tumors. Clear cell renal cell carcinoma (ccRCC) constituted the predominant histological subtype, accounting for 87.6% of all cases, while 79.6% of the tumors were categorized as pathological stage T1 according to the TNM staging system. Regarding treatment modalities, the utilization rates of radical nephrectomy and partial nephrectomy were observed to be nearly equivalent. A detailed demographic and clinical characterization of the patient population is presented in Table 1. The patients’ geographic area distribution is revealed in Fig. 1.
Table 1 Characteristic of patient population (N = 9110)Fig. 1
Patients’ geographic area distribution
Our urologic oncology was staffed by 15–20 surgeons subspecializing in kidney cancer (2013–2022). Procedures were performed or supervised by these surgeons, organized into laparoscopic, open and robotic surgery teams to leverage expertise. 20–35 surgical residents assisted as first assistants without primary operative roles. Cases were allocated by tumor complexity and surgeon proficiency, with a rotating schedule capping individual workloads at 10–20 cases/week to ensure quality and prevent overload.
Decadal trend analysisVariability in the number of surgical proceduresOver the past decade, there had been a consistent increase in the number of patients eligible for nephrectomy, indicating a rising demand for surgical interventions. Notably, the year 2020 showed deviations primarily attributable to the effects of the global health crisis. However, beginning in 2019, the annual number of individuals undergoing surgery had consistently exceeded one thousand cases (Fig. 2).
Fig. 2
Trends in the number of surgical operations for RCC patients
Alterations in age and genderThe median age of onset for operable RCC had remained stable, falling within the range of 54 to 57 years. A longitudinal analysis conducted over the past decade, with a focus on the median age, reveals no discernible trend toward either younger or older ages among patients undergoing surgical treatment for RCC. This consistency indicated that the demographic profile of individuals requiring surgical intervention for RCC had largely remained unchanged during the observed period (Fig. 3).
Fig. 3
Trends in the age of RCC patients. * RCC, renal cell carcinoma; PSM, positive surgical margin
A trend analysis was performed to evaluate the age distribution of 9,110 RCC patients across five distinct biennial periods: 2013–2014, 2015–2016, 2017–2018, 2019–2020, and 2021–2022. The analysis demonstrated that the median age of patients varied slightly, ranging between 55 and 57 years across these intervals. However, this fluctuation was not statistically significant (P = 0.225), suggesting that the age distribution of patients undergoing surgical treatment for RCC has remained relatively stable over the examined decade (Table 2).
Table 2 Comparison of the age composition of RCC patients in five periodsSurgical approachesBetween 2013 and 2015, a marked preference for partial nephrectomy was observed, with approximately 70% of patients opting for this surgical approach. Following this period, the proportion of partial nephrectomies underwent a gradual decline, characterized by intermittent fluctuations. Currently, the distribution between partial nephrectomy and radical nephrectomy has reached a state of equilibrium (Fig. 4).
Fig. 4
Trends in the surgical approaches of RCC patients
Surgical modalitiesThroughout the decade from 2013 to 2022, laparoscopic surgery remained the predominant surgical modality, though its proportion showed some fluctuation. Open surgery experienced a consistent decline, decreasing from over 20% in 2013 to below 10% by 2022. Concurrently, robotic-assisted surgery, starting from a negligible proportion, demonstrated a significant and rapid increase in utilization, particularly in the latter half of the decade, reaching over 20% by 2022 (Fig. 5).
Fig. 5
Trends in the surgical modalities of RCC patients
Pathological T (pT) stagesDecade-long postoperative pathological analyses consistently demonstrated a predominant prevalence of pT1 stage tumors, accounting for 78.0% to 84.2% of all cases. In contrast, pT2, pT3, and pT4 stage tumors were significantly less frequent, representing 3.2% to 5.6%, 10.9% to 19.1%, and 0% to 0.8% of cases, respectively (Fig. 6). Over this ten-year timeframe, the proportional distribution of pT stages exhibited some variability. However, this fluctuation did not follow any clear or consistent trend (Table 3).
Fig. 6
Trends in the T stages of RCC patients
Table 3 Comparison of the pT stages of RCC patients in five periodsTumor diametersIn the assessment of trends in average tumor diameters among patients with RCC undergoing surgical intervention, stratified into five-year intervals, the mean tumor diameters for the periods 2013–2014, 2015–2016, 2017–2018, 2019–2020, and 2021–2022 were recorded as (4.21 ± 2.47) cm, (4.38 ± 2.37) cm, (4.16 ± 2.28) cm, (4.05 ± 2.35) cm, and (3.83 ± 2.37) cm, respectively. These data indicated a noticeable trend of gradual reduction in tumor diameters over time among RCC patients undergoing surgery during the past decade, with statistically significant differences (P < 0.001) (Fig. 7).
Fig. 7
Trends in the tumor diameters of RCC patients
Pathological classificationsOver the past decade, ccRCC had predominated in the pathological classification of RCC, accounting for 86.3% to 89.7% of all diagnosed cases (Fig. 8). Notably, the proportion of pathological subtypes among patients undergoing surgical treatment for RCC had remained remarkably consistent, with no significant variations observed in the distribution of these classifications (P = 0.162) (Table 4).
Fig. 8
Trends in the pathological classifications of RCC patients
Table 4 Comparison of the pathological classifications of RCC patients in five periodsPositive surgical margin (PSM) ratesA significant downward trend in PSM rates was observed among surgically treated RCC patients over the past decade (P < 0.001) at our institution (Table 5), despite interim fluctuations (Fig. 9).
Table 5 Comparison of the PSM rates of RCC patients in five periodsFig. 9
Trends in the positive surgical margin rates of RCC patients
Correlation between demographic characteristics and postoperative pathological outcomesGenderThe analysis of gender-based differences in surgical approaches and subsequent pathological findings uncovered significant distinctions. A markedly higher percentage of female patients underwent radical nephrectomy compared to male patients, with this difference being statistically significant (P < 0.001). Additionally, a notable association was observed between gender and the prevalence of specific pathological subtypes of RCC, with a significantly greater proportion affecting female patients (P < 0.001). However, no significant gender-related differences were detected regarding the number of primary lesions (P = 0.394) or pT-stage classification (P = 0.165) (Table 6).
Table 6 Gender-based comparison of surgical method, number of primary lesions, pathological types, and pT staging in RCC PatientsAgeThe patients treated in our center were stratified into three distinct age groups: "Under 18," "18–64," and "65 and older." We conducted an analysis of differences in surgical characteristics and pathological outcomes among these groups.
Our comparative findings revealed significant variations in surgical approaches (P < 0.001), pT-stage classification (P < 0.001), and pathological subtypes (P < 0.001) across the different age categories. Notably, a higher proportion of patients aged 18–64 underwent partial nephrectomy compared to those aged 65 and older (P < 0.001). In contrast, among patients under 18, a greater fraction underwent radical nephrectomy and were diagnosed with specific pathological subtypes, which may be associated with more advanced pT-stage disease (P < 0.001). However, the disparity in the number of primary foci among the three age groups did not reach statistical significance (P = 0.077) (Table 7).
Table 7 Age-based comparison of surgical method, number of primary lesions, pathological types, and pT staging in RCC PatientsCorrelation between pathological types, demographic characteristics, and stagingThe analytical results indicated that the pT staging in non-ccRCC cases tends to be more advanced compared to ccRCC (P < 0.001). Nevertheless, no significant difference was observed in the number of primary lesions across various pathological types (P = 0.057) (Table 8).
Table 8 Comparison of the composition ratio of the number of primary lesions and pT staging in patients undergoing surgery for different pathological types of RCCFurthermore, within this cohort, a subset of 79 patients (0.87%) was identified as having Xp11.2 translocation RCC, which belongs to the MiTF/TFE3 family of transcription factor fusion renal tumors. A marked gender disparity was observed, with females constituting the majority at 49 cases (62.0%), compared to males who accounted for 30 cases (38.0%). The median age at diagnosis within this subgroup was 32 years (range: 15–89 years), with a mean age of 35.86 years (standard deviation ± 3.48 years). Notably, the age of onset for patients with Xp11.2 translocation RCC was significantly younger than that of the broader RCC patient population treated at this institution (P < 0.001).
Comments (0)