
Remember me


This study analyzed the distribution of sex and age across the RA, disease control, and healthy control groups. Regarding gender distribution (Fig. 3A), female patients significantly outnumbered males in the RA group (206 females vs. 51 males). A similar trend was observed in the disease control group (145 females vs. 72 males). In contrast, the healthy control group exhibited a more balanced gender distribution (22 females vs. 18 males). Regarding age distribution (Fig. 3B), the mean age of the RA group (58.22 ± 11.61 years) was than that observed in the disease control group (46.24 ± 13.38 years) and the healthy control group (39.50 ± 14.19 years) (Table 1).
Fig. 3
Gender distribution and age comparison of RA patients. Note A Bar chart showing the gender distribution in the RA group, disease control group, and healthy control group; B bar chart showing the mean age of the RA group, disease control group, and healthy control group. p < 0.01: **; p < 0.0001: ****
Table 1 Patient Characteristics of the studyComparison of the diagnostic value of anti-MCV, anti-CCP, and RF in RAIndividuals with confirmed RA were defined as test-positive cases, and individuals in the disease control and healthy control groups were considered test-negative. The diagnostic efficacy of anti-MCV, anti-CCP, and RF was assessed through ROC curve analysis, including AUC, sensitivity, and specificity (Fig. 4A; Table 2). The AUCs for anti-MCV, anti-CCP, and RF were 0.911 (95% CI 0.872–0.934), 0.858 (95% CI 0.812–0.886), and 0.884 (95% CI 0.842–0.908), respectively. Statistical comparison using DeLong’s test indicated no significant difference between the performances of anti-MCV and anti-CCP (p = 0.073). The combination of all three markers increased the AUC to 0.932 with a sensitivity of 89.1% (Fig. 4B).
Fig. 4
ROC curve analysis of anti-MCV, anti-CCP, and RF in RA diagnosis
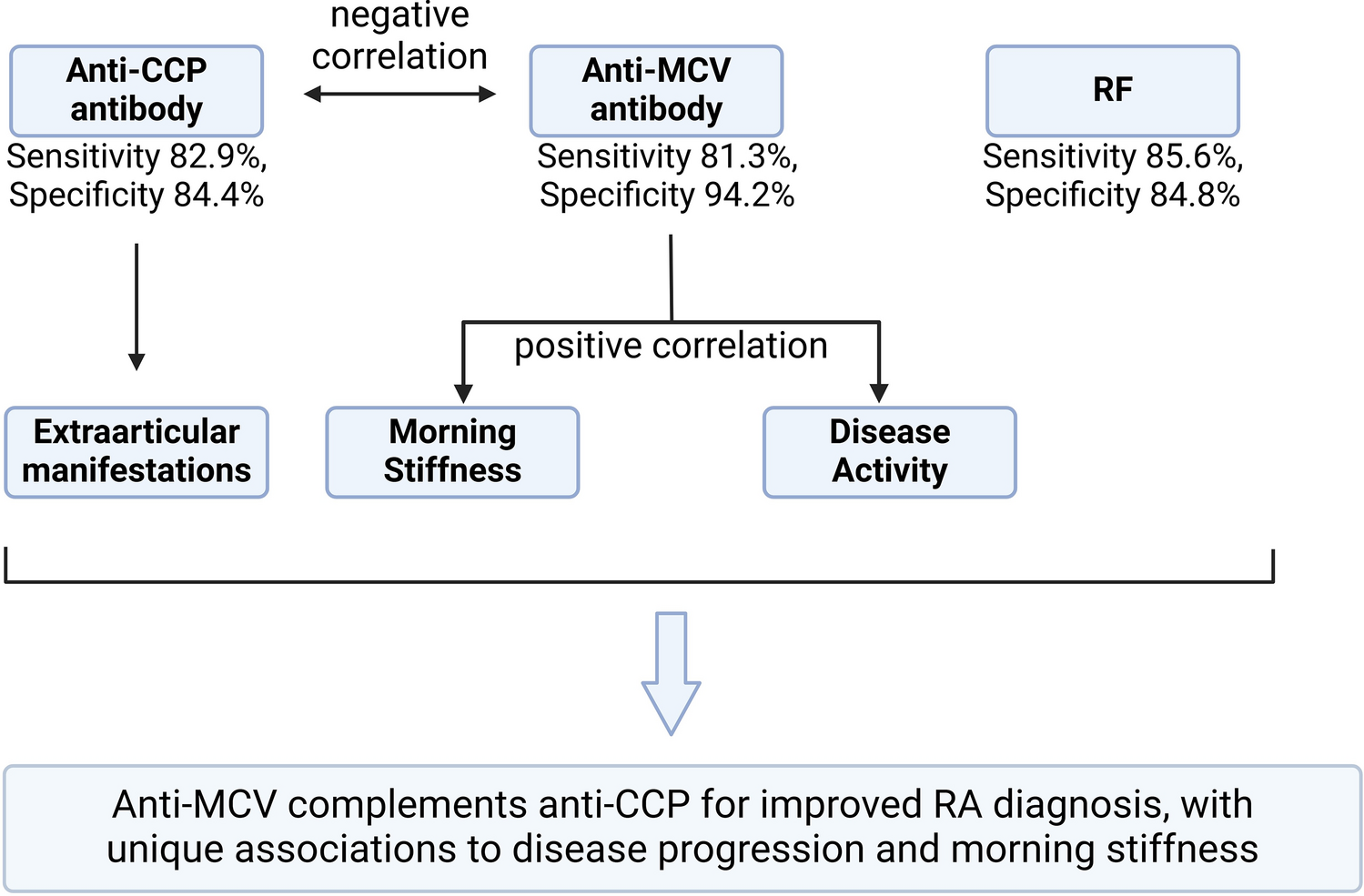
Table 2 Diagnostic efficacy of anti-MCV, Anti-CCP, and RF for RAIn subgroup analyses, anti-CCP antibodies showed the highest AUC for differentiating RA from healthy controls (0.96, 95% CI 0.93–0.99; Fig. 4C), whereas anti-MCV antibodies demonstrated better performance in distinguishing RA from other autoimmune diseases (AUC = 0.87, 95% CI 0.83–0.91; Fig. 4D). At the optimal cutoff defined by the Youden index, the sensitivity of anti-MCV was 82.9%, slightly higher than that of anti-CCP (81.3%, p > 0.05) and slightly lower than RF (85.6%, p > 0.05). Anti-CCP demonstrated superior performance (94.2%), which was significantly higher than that of anti-MCV (84.4%) and RF (84.8%).
Multivariate logistic regression adjusted for age and sex showed that anti-MCV antibody positivity had the strongest association with RA diagnosis (aOR = 8.42, 95% CI 5.67–12.51), followed by anti-CCP (aOR = 7.15, 95% CI 4.89–10.45) and RF (aOR = 6.83, 95% CI 4.62–10.10; Table 3). Covariate-adjusted ROC analysis yielded AUCs of 0.903 (anti-MCV), 0.849 (anti-CCP), and 0.875 (RF), with a < 3% deviation from unadjusted values, indicating the robustness of the findings.
Table 3 Regression analysis for diagnostic performance of antibodies after adjustmentSignificant correlation between anti-MCV antibody and morning stiffness in RA patientsA robust association was identified between anti-MCV antibody positivity and the occurrence of morning stiffness among RA patients. Among anti-MCV-positive patients, 85 reported morning stiffness, while 25 did not. In contrast, among anti-MCV-negative patients, 96 reported morning stiffness, and 51 did not. Chi-square analysis revealed a statistically meaningful relationship between anti-MCV positivity and morning stiffness symptoms (p < 0.05; Fig. 5). The prevalence of morning stiffness was 77.3% (85/110) in the anti-MCV-positive group and 65.3% (96/147) in the anti-MCV-negative group (Table 4). Stratified analysis by age (median split at 50 years) showed that the association remained significant in both subgroups (≤ 50 years: 76.5%, p = 0.021; > 50 years: 78.1%, p = 0.042). Multivariate logistic regression adjusted for age, anti-MCV positivity remained independently associated with morning stiffness (aOR = 1.89, 95% CI 1.21–2.95, p = 0.005; Table 5).
Fig. 5
Relationship between anti-MCV antibody and morning stiffness in RA patients. Note Bar chart showing the distribution of morning stiffness in anti-MCV antibody-positive and negative groups. The difference between the two groups was statistically significant (χ2 = 4.326, p = 0.038). p < 0.05: *
Table 4 Relationship between anti-MCV and morning stiffness in RATable 5 Age-stratified and covariate-adjusted analysis of the association with morning stiffnessCorrelation between anti-MCV antibody and disease duration, CRP, bone mineral density (BMD), and 28-joint disease activity score (DAS28)The correlations between anti-MCV antibody levels and clinical parameters in RA patients, including disease duration, CRP, ESR, BMD, and DAS28, were analyzed (Table 6). Anti-MCV levels showed a weak but statistically significant negative correlation with disease duration (r = − 0.057, p < 0.05), CRP (r = − 0.047, p < 0.05), and ESR (r = − 0.053, p < 0.05), implying that elevated antibody titers may be modestly linked to shorter disease history and reduced systemic inflammatory markers. No meaningful associations were detected between anti-MCV levels and BMD or DAS28 scores (p > 0.05). Although statistically significant, the observed correlation coefficients were all well below the threshold for clinical relevance (|r|≥ 0.3), indicating that anti-MCV levels may have limited utility in assessing bone status or overall disease activity in RA.
Table 6 Correlation between anti-MCV and disease duration, CRP, BMD, and DAS28 in RAInterrelationships among anti-MCV, anti-CCP, and RF in RA diagnosisThe relationships among anti-MCV, anti-CCP antibodies, and RF were evaluated by comparing their individual and combined positivity rates in RA patients (Fig. 6; Table 7). There was no significant difference in positivity between anti-MCV alone and anti-CCP alone (\(\chi_^\) = 2.332, p1 = 0.128), or between anti-MCV alone and RF alone (\(\chi_^\) = 3.332, p2 = 0.068)), indicating similar diagnostic detection capabilities for each marker. Triple positivity involving all three antibodies (MCV+/CCP+/RF+) showed the highest detection rate (68.09%), which was significantly higher than MCV+/CCP+ (p = 0.016), MCV+/RF+ (p = 0.009), and CCP+/RF+ (p = 0.021). These findings suggest that triple-antibody testing substantially increases the diagnostic yield compared to dual- or single-marker combinations.
Fig. 6
Interrelationships among anti-MCV antibody, anti-CCP antibody, and RF in RA patients. Note This figure illustrates the positive rates of antibody combinations in RA patients
Table 7 Interrelationships among three antibodiesNegative correlations among anti-MCV, anti-CCP, and RF in RA patientsTo assess the associations among anti-MCV, anti-CCP antibodies, and RF in RA patients, correlation analysis was conducted (Table 8). A significant negative correlation was observed between anti-MCV and anti-CCP antibody levels (r = − 0.470, p < 0.05), as well as between anti-MCV and RF levels (r = − 0.231, p < 0.05). These results indicate that higher levels of anti-MCV antibodies were associated with lower levels of anti-CCP antibodies and RF.
Table 8 Relationship between anti-MCV, anti-CCP, and RFAssociation between anti-MCV, anti-CCP, RF, and extra-articular manifestations and overlap syndromes in RA patientsThis study analyzed clinical data from 257 patients with RA to examine the associations of anti-MCV, anti-CCP antibodies, and RF with extra-articular manifestations and overlap syndromes. Extra-articular involvement was observed in 156 patients (60.7%), including pulmonary involvement in 42 cases (16.34%), hematologic abnormalities in 100 cases (38.91%), and renal involvement in 4 cases (1.56%). Sixteen patients (6.23%) were diagnosed with overlap syndromes involving other autoimmune diseases, including SS (7 cases), undifferentiated connective tissue disease (3 cases), SLE (2 cases), autoimmune liver disease (3 cases), and polymyositis (1 case). Chi-square analysis revealed that anti-CCP antibody seropositivity was linked to the presence of extra-articular features (χ2 = 9.245, p < 0.05), whereas no statistically meaningful associations were detected for anti-MCV or RF (p > 0.05). None of the three antibodies demonstrated a reliable relationship with overlap syndromes (p > 0.05) (Fig. 7; Table 9). Although anti-MCV antibodies were not significantly associated with overall extra-articular involvement, subgroup analysis suggested differential distribution in specific complications such as interstitial lung disease and cardiovascular events (Table 10). RF showed no significant association with extra-articular manifestations or overlap syndromes.
Fig. 7
Relationship between anti-MCV antibody, anti-CCP antibody, RF, extra-articular manifestations, and overlap syndromes in RA patients. Note A Distribution of extra-articular manifestations in anti-MCV antibody, anti-CCP antibody, and RF positive and negative groups; B distribution of overlap syndromes in anti-MCV antibody, anti-CCP antibody, and RF positive and negative groups. p < 0.01: **; not significant: “ns”
Table 9 Relationship between three autoantibodies and extra-articular manifestations and overlap syndromes in RATable 10 Association between anti-MCV antibody and organ-specific extra-articular manifestations in RA patients
Comments (0)