Combination chelation therapy has been used to improve outcomes if monotherapy proves inadequate to control iron overload, particularly in the heart and liver. Most commonly used regimes give DFP daily at standard doses, combined with varying frequency and dosing of DFO [1]. More recently, combinations of DFX with DFO, or DFX with DFP have been evaluated [2, 3]. Our study has shown significant improvement in Serum ferritin within 6–12 months with a significant decrease in serum ferritin within these relatively short time points. Recent studies have suggested combination of deferasirox and deferiprone to be an effective regimen [4,5,6,7]. Previously studies showed clinical improvement with combination of desferoxamine and deferiprone in cardiac and endocrine complications of iron overload in 52 patients not responding to single chelator use [8]. Combination of deferiprone with subcutaneous desferoxamine was more effective to lower serum ferritin and improved echocardiographic parameters with no statistically significant differences in mortality or cost between the groups [9,10,11]. Though this method of combined chelation remains the gold standard and recommended method for heavily iron-overloaded patients, it does not lend itself to ease of administration and hence poor adherence. This is especially true in the developing world where cost of care if often borne by the parents. Two oral chelators used in this study was well accepted and well tolerated.
The increased risk of sinusoidal obstruction syndrome in iron-overloaded patients with thalassemia undergoing an allogeneic stem cell transplant is well documented [12, 13]. With accessibility to curative options for stem cell transplant improving in the developing world also, optimal iron chelation prior to transplant is important. In this setting, a regimen with improved adherence, and equal efficacy is preferred.
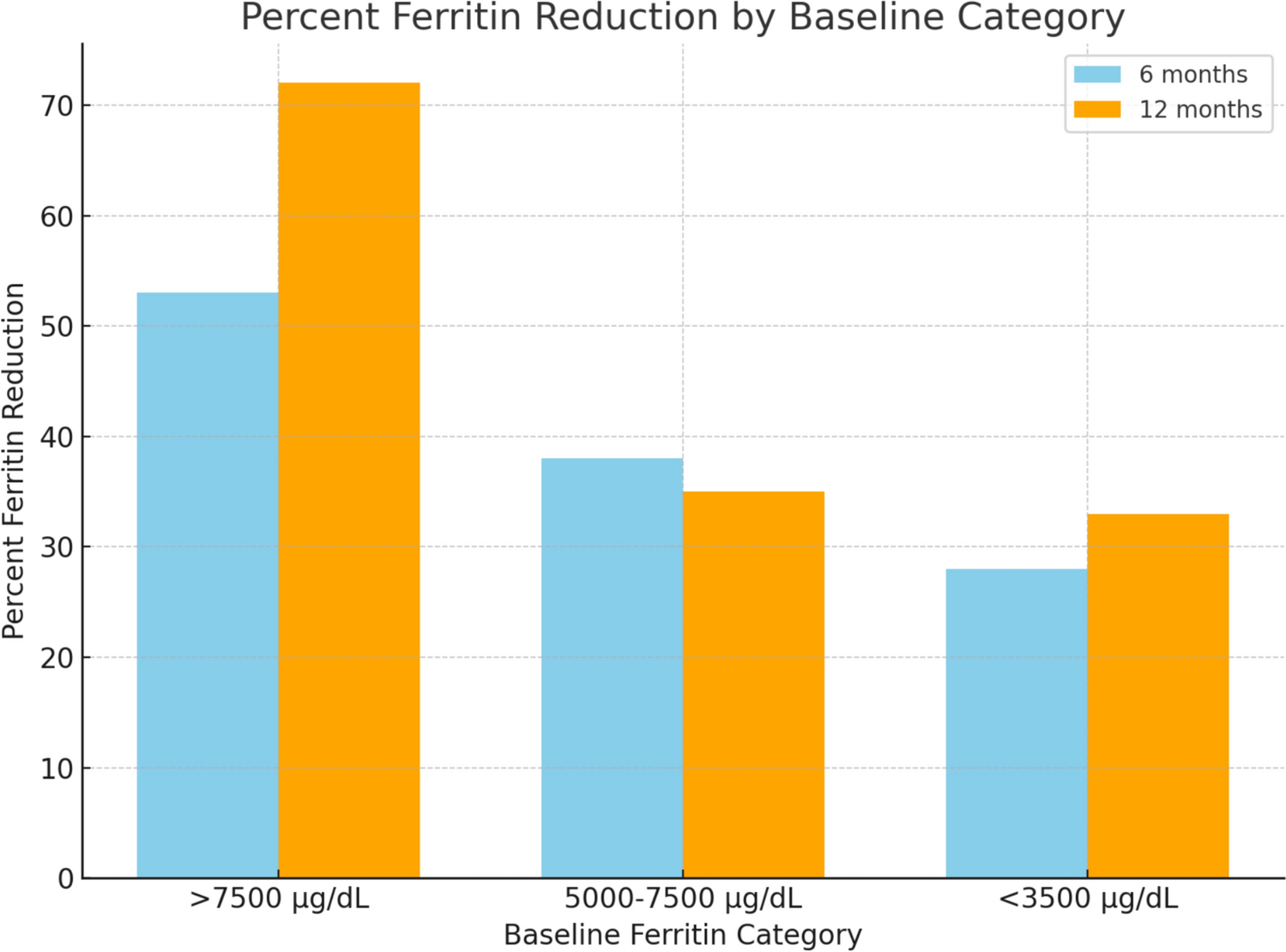
Though desferioxamine has been the gold standard in iron chelation, studies have demonstrated comparable amounts of iron excretion when deferiprone was compared to desferoxamine [14, 15]. Deferiprone results in more significant reduction in iron levels in those with a higher iron burden [16]. It is interesting to note that in our study those with a higher serum ferritin level had a proportionately greater drop in serum ferritin. This observation is similar in other studies on combination of DFP and DFX [16]. The major limitation of our study is the inaccessibility to T2* MRI due to high cost for most of our patients. This limitation notwithstanding, the trend of serum ferritin showing statistically significant decreases is reassuring. We acknowledge that T2 MRI* is the gold standard for assessing iron overload in organs such as the heart and liver. However, due to resource constraints in developing and underdeveloped countries, access to T2 MRI is limited* and often unavailable for routine monitoring in many clinical settings, including ours.
Given these limitations, serum ferritin remains the most widely used and accessible biomarker for assessing iron burden in resource-limited settings. While it has known variability and is influenced by factors such as inflammation, it still provides valuable trends in iron overload management and is routinely used in clinical decision-making.
As a retrospective audit, this study aimed to evaluate the practical efficacy and safety of combination therapy in a cohort that required it. While a randomized controlled trial (RCT) or a matched control study would provide higher-level evidence, real-world audits are critical in resource-limited settings to guide treatment modifications. Instead of a control group, we used baseline pre-treatment serum ferritin levels and trends over time as internal references to assess efficacy. This allowed us to demonstrate the impact of combination therapy within the patient population, reducing variability due to interpatient differences.
Combination oral therapy is an effective, acceptable and cheaper mode of chelation therapy which may be utilized as a method of chelation in developing countries where iron burden is high [6, 7, 16, 17].



Comments (0)