Traditional biomarkers in septic cardiomyopathy
Cardiac biomarkers play a key role in the assessment of myocardial injury and dysfunction across a wide range of clinical settings. In the context of sepsis, however, their interpretation is particularly challenging. Sepsis induces profound changes in cardiovascular physiology, including inflammatory-driven myocardial depression, vasoplegia, and microcirculatory failure. These systemic abnormalities can lead to elevations in biomarkers commonly used to detect acute coronary syndromes or heart failure, even in the absence of primary heart disease [18,19,20,21].
In septic cardiomyopathy (SCM), traditional cardiac biomarkers, such as troponins and natriuretic peptides, are frequently elevated, but their specificity for SCM remains limited [18,19,20,21]. Moreover, sepsis itself may interfere with biomarker kinetics through mechanisms such as impaired clearance (e.g., due to renal dysfunction), altered tissue release, and systemic inflammation. Despite these limitations, these biomarkers remain widely used because of their availability, rapid half-life, and long-standing clinical familiarity [2, 3, 28].
Cardiac troponins
Cardiac troponins (cTnI and cTnT) are regulatory proteins of the troponin complex, which are involved in cardiomyocyte contractility. Cardiac troponin I (cTnI) and troponin T (cTnT) are both components of the troponin complex specific to cardiac muscle, but they differ in structure and assay characteristics. cTnI is exclusively expressed in cardiac tissue and is highly specific for myocardial injury, while cTnT, although also cardiac-specific, may show slight cross-reactivity in certain conditions. Both are encoded by cardiac-specific genes and are released into circulation following myocardial cell injury [29]. Troponins are released into the bloodstream following cardiomyocyte injury [29]. These markers are considered the gold standard for detecting myocardial injury [29]. Elevated troponin levels are common in patients with sepsis and have been associated with increased mortality, longer intensive care unit (ICU) stays, and greater incidence of organ dysfunction [18, 19]. However, the mechanisms underlying troponin release in sepsis are multifactorial and not necessarily linked to myocardial ischemia. Proposed mechanisms include cytokine-mediated cardiomyocyte injury, oxidative stress, mitochondrial dysfunction, and membrane leakage [18].
The diagnostic value of troponins in SCM is limited by their low specificity. Troponin elevations can occur in a variety of conditions including renal failure, pulmonary embolism, and tachyarrhythmias, all of which may coexist in septic patients [30,31,32,33]. Moreover, the degree of troponin elevation does not correlate reliably with the severity of myocardial dysfunction assessed by echocardiography [13, 16, 34]. This hampers their utility in differentiating SCM from other causes of cardiac biomarker elevation [32, 33].
Nonetheless, troponin measurements have prognostic relevance [30,31,32,33,34,35]. Several studies showed that elevated troponins in sepsis are independently associated with increased mortality, even in the absence of overt cardiac dysfunction [18, 19, 30,31,32,33,34,35]. Serial measurements may also provide dynamic information on myocardial stress or recovery, although this did not reach yet standard practice.
Brain natriuretic peptide and NT-proBrain natriuretic peptide
Brain natriuretic peptide (BNP) and its inactive fragment proBrain natriuretic peptide (NT-proBNP) belong to the vasoactive peptide family and are derived from the cleavage of a common precursor, proBNP, into active BNP and inactive NT-proBNP. These peptides are secreted by cardiomyocytes in response to ventricular wall stretch and volume overload. In sepsis, both markers are frequently elevated, reflecting myocardial strain and fluid shifts rather than classic heart failure [36]. Like troponins, BNP and NT-proBNP levels correlate with disease severity and prognosis, and their elevation has been linked to increased mortality and ICU length of stay [21, 37, 38].
The interpretation of natriuretic peptides in sepsis is limited by multiple confounding factors [20, 37]. Renal dysfunction, common in septic patients, impairs peptide clearance, particularly for NT-proBNP [38, 39]. Moreover, systemic inflammation and vasodilation can alter ventricular loading conditions, leading to elevated levels without overt systolic dysfunction. Studies investigating the relationship between BNP/NT-proBNP and echocardiographic findings of SCM have yielded inconsistent results [40]. Nonetheless, these biomarkers may still have a role in the early identification of septic patients at risk of cardiovascular compromise [37, 38]. When combined with echocardiographic assessment and clinical context, natriuretic peptides may contribute to risk stratification and guide fluid or vasopressor management [40].
Other classical markers: CK-MB, LDH, and myoglobin
Before the widespread use of cardiac troponins and natriuretic peptide assay, several other biomarkers were commonly measured to assess myocardial injury. Among these, creatine kinase-MB (CK-MB), lactate dehydrogenase (LDH), and myoglobin were historically considered part of the standard cardiac panel. However, their utility in SCM is now limited due to low specificity, poor sensitivity, and significant overlap with other causes of systemic illness [41].
CK-MB is an isoenzyme predominantly found in cardiac muscle, but it is also present in skeletal muscle. It plays a role in cellular energy metabolism and is released into the bloodstream following muscle cell damage. In sepsis, CK-MB levels may rise due to global muscle injury, rhabdomyolysis, or increased cellular turnover, making it an unreliable indicator of myocardial-specific damage. Its shorter half-life and susceptibility to noncardiac influences further diminish its diagnostic value in the septic context [41, 42].
LDH is a ubiquitous intracellular enzyme released during cell lysis and tissue injury. While elevated LDH may reflect ongoing cellular damage in sepsis, it lacks organ specificity and does not provide actionable information about cardiac involvement [42, 43]. Its levels are influenced by hemolysis, hepatic dysfunction, and malignancies, all of which may coexist with sepsis.
Myoglobin, a heme protein released from both cardiac and skeletal muscle, rises rapidly after injury, but is cleared quickly through the kidneys. In septic patients, myoglobin levels can be elevated due to noncardiac muscle damage or renal impairment, limiting its interpretability. Its lack of specificity and rapid kinetics make it largely obsolete in modern critical care settings [43].
Although these markers may still be listed in some laboratory panels, especially in resource-limited settings, their clinical relevance in the diagnosis or prognostication of SCM is minimal. They are not recommended as stand-alone indicators of myocardial dysfunction and should not guide clinical decision-making in isolation.
Emerging biomarkers in septic cardiomyopathy
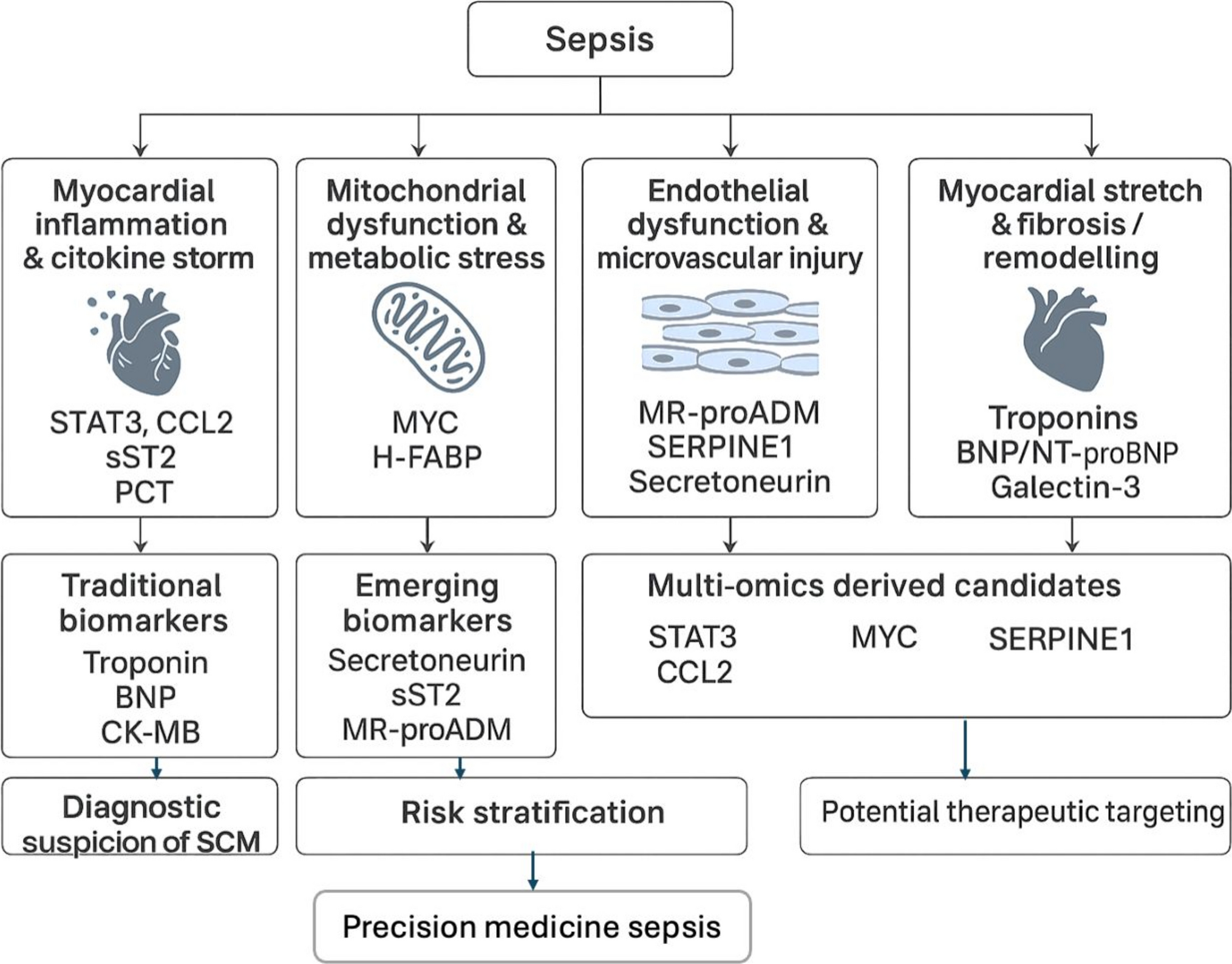
Recent advances in molecular biology and high-throughput technologies have led to the discovery of a growing number of novel markers with potential applications in the diagnosis, monitoring, and prognostication of SCM [44, 45]. These emerging indicators reflect various pathophysiological pathways, including inflammation, oxidative stress, myocardial stretch, endothelial activation, and immune dysregulation. Unlike traditional biomarkers, which largely indicate cardiac injury or wall stress, many of these new markers aim to capture the early and dynamic processes of septic myocardial dysfunction [8, 46]. The main promise of these novel markers lies in their potential for earlier detection of SCM, improved prognostic accuracy, and, in some cases, mechanistic insights that could support therapeutic targeting [46]. However, most of them remain confined to the research setting, with limited validation in large-scale, multicenter cohorts. Additionally, significant heterogeneity in study design, timing of sampling, assay platforms, and echocardiographic definitions of SCM hampered their clinical translation.
In the following sections, we review the most relevant and promising emerging biomarkers, with a focus on their biological rationale, current evidence, and limitations in the context of SCM (further summarized in Table 1).
Table 1 Overview of emerging biomarkers in septic cardiomyopathySecretoneurin
Secretoneurin is a neuropeptide derived from chromogranin/secretogranin proteins, produced by neuroendocrine and cardiac cells, and involved in calcium signaling, inflammation, and endothelial function. It has emerged as a potential cardiovascular biomarker, particularly in critically ill patients, where elevated levels have been associated with increased mortality, arrhythmia risk, and myocardial dysfunction [47,48,49].
In sepsis, secretoneurin levels appear to correlate with disease severity and may reflect early cardiac involvement. A few studies have shown that it rises in parallel with troponins and BNP, but may offer additional prognostic value due to its distinct pathophysiological signature. Importantly, it may act as both a marker and a mediator of myocardial stress via calcium dysregulation and endothelial activation [47, 48]. However, clinical data on secretoneurin in SCM remain limited. The marker has not yet been validated for routine use, and compared to established biomarkers its performance is still under investigation.
Soluble suppression of tumorigenicity-2 (sST2)
sST2 is a member of the interleukin-1 receptor family, released by cardiomyocytes and immune cells in response to mechanical strain and inflammation [50]. It acts as a decoy receptor for IL-33, disrupting cardioprotective signaling and promoting myocardial remodeling and fibrosis. In heart failure, sST2 is a well-established prognostic biomarker, included in some risk stratification algorithms [51].
In sepsis, sST2 levels are frequently elevated and correlate with both disease severity and mortality. Several studies have suggested that sST2 may help identify patients at risk for septic cardiomyopathy, particularly when used in combination with echocardiographic assessment. Unlike natriuretic peptides, sST2 is less affected by age, body mass, and renal function, which may confer an advantage in critically ill populations [52,53,54,55,56].
Nevertheless, its role as a specific marker of SCM remains to be validated. The lack of cardiac specificity and its modulation by systemic inflammation may limit its stand-alone diagnostic value.
Presepsin (PSP)
PSP, also known as soluble CD14 subtype (sCD14-ST), is a fragment released by monocytes and macrophages during bacterial phagocytosis. It is part of the innate immune response and belongs to the pattern recognition receptor family [56]. It has been widely studied as an early diagnostic marker for sepsis and as a potential prognostic tool [56,57,58,59].
While not specific to cardiac dysfunction, some studies have found associations between PSP levels and myocardial depression in septic patients [60]. These findings suggest that it may reflect the interplay between innate immune activation and organ dysfunction, including the heart [60,61,62].
However, its utility in identifying SCM is likely indirect. The elevation of PSP reflects the septic state itself rather than myocardial-specific pathophysiology. It may play a complementary role when interpreted in conjunction with cardiac biomarkers and imaging.
Procalcitonin (PCT)
Procalcitonin is a prohormone of calcitonin, normally produced by thyroid C cells but also expressed in various tissues during systemic bacterial infection [63]. It is a widely used marker of bacterial infection and systemic inflammation, especially in guiding antibiotic therapy [63]. It is not a cardiac biomarker per se but is frequently included in sepsis panels. Some studies have examined the relationship between PCT levels and cardiac dysfunction in sepsis, with conflicting results [64]. While elevated PCT may reflect disease severity and correlate with worse outcomes, it does not provide direct information about myocardial involvement [56, 63, 64]. Moreover, it is heavily influenced by infection burden, renal function, and timing of measurement [63].
In the context of SCM, PCT may serve as a general marker of systemic burden but lacks the specificity or mechanistic relevance needed for targeted cardiac assessment.
Mid-regional pro-adrenomedullin (MR-proADM)
Adrenomedullin is a vasodilatory peptide with roles in endothelial barrier function, vascular tone, and microcirculatory integrity. MR-proADM is a stable surrogate for biologically active adrenomedullin and is gaining attention as a prognostic marker in sepsis [59, 65, 66].
In patients with septic shock, elevated MR-proADM levels correlate with endothelial dysfunction, organ failure, and mortality. Recent data suggest a potential link with myocardial dysfunction. This may be mediated through microvascular hypoperfusion and capillary leak. [67, 68].
Though not cardiac-specific, MR-proADM may reflect global cardiovascular stress and hemodynamic instability. Its role in SCM is still exploratory but potentially valuable, particularly when integrated into multimodal risk scores.
Heart-type fatty acid-binding protein (H-FABP)
H-FABP is a small cytoplasmic protein abundant in cardiomyocytes, part of the fatty acid-binding protein family, released rapidly after myocardial injury. Its kinetics are faster than troponin, making it attractive for early detection of cardiac damage [69].
In sepsis, elevated H-FABP levels have been associated with myocardial dysfunction and increased mortality [70, 71]. It may outperform troponins in identifying early myocardial involvement, especially when troponin levels remain within the normal range [67, 72]. However, its interpretation can be challenging due to renal clearance and possible elevation from noncardiac muscle injury.
Although promising, H-FABP is not yet widely available and lacks standardized thresholds for SCM.
Calprotectin (S100A8/A9)
Calprotectin is a neutrophil-derived alarmin released early in the inflammatory cascade, with plasma levels > 2–3 mg/L shown to differentiate sepsis from sterile inflammation and correlate with illness severity and multi-organ dysfunction [73]. While its role as a general sepsis biomarker is well supported by recent studies, evidence specific to cardiac involvement remains limited. A single-center cohort reported an association between high calprotectin levels and left ventricular systolic dysfunction [74], and in experimental models, pharmacologic inhibition or gene knockout of S100A8/A9 reduced myocardial depression and inflammation [73]. The proposed mechanism involves TLR4/RAGE signaling and mitochondrial dysfunction, but its direct cardiotropic role in humans rema



Comments (0)