
Remember me
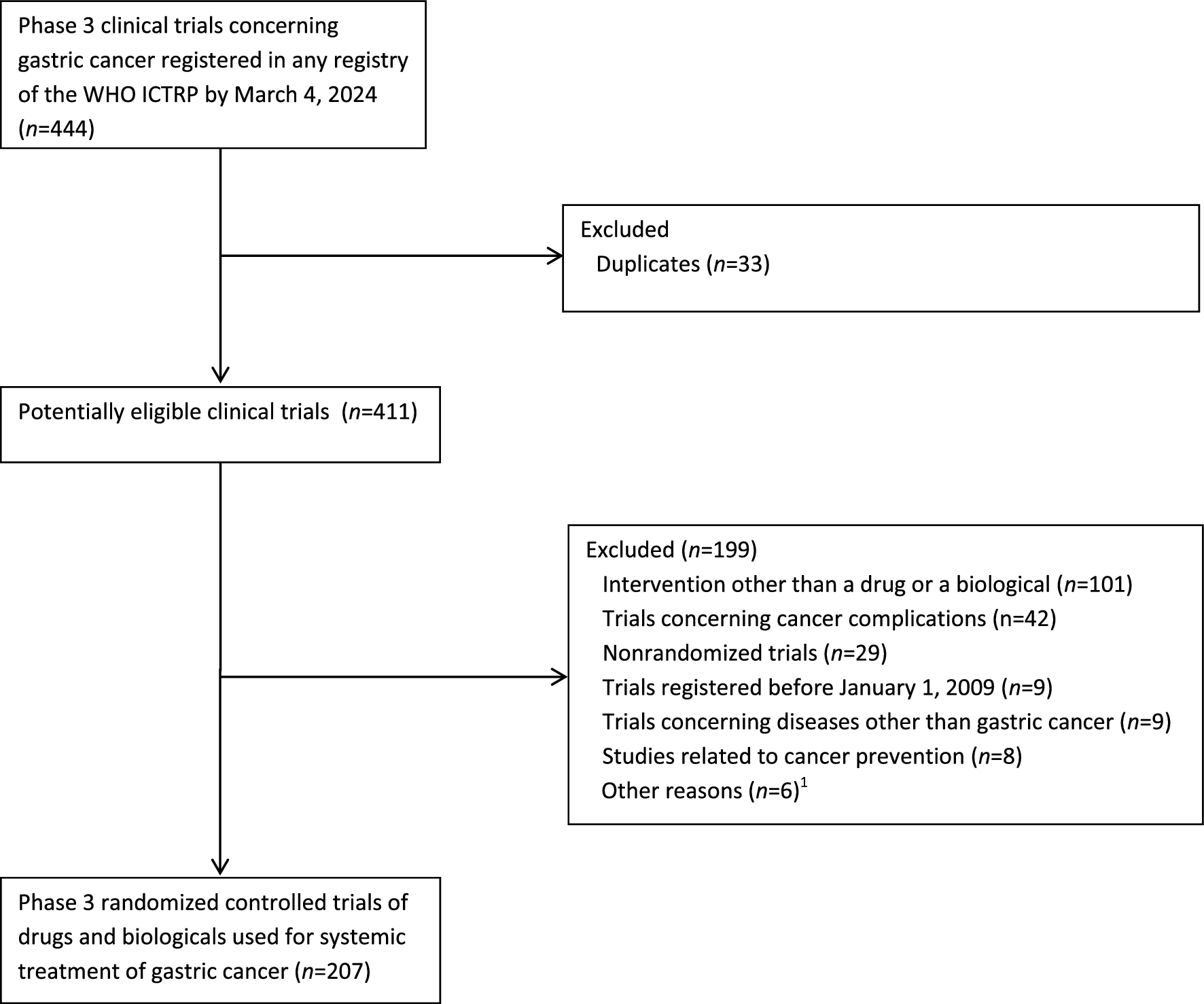

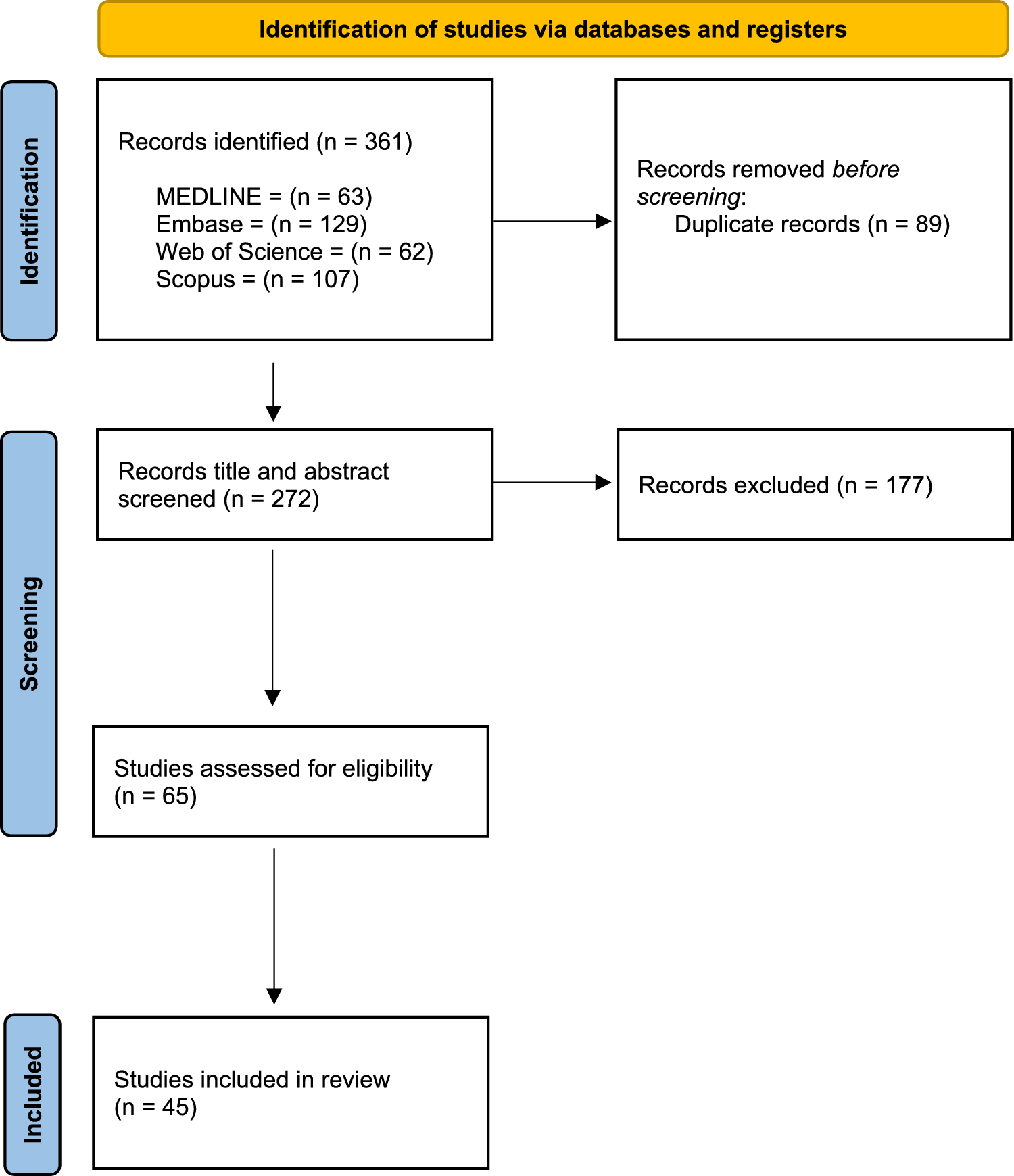
Selection of eligible RCTs is shown in Fig. 1. The initial search in the WHO ICTRP yielded 444 trials. The most common reason for a trial’s exclusion was the use of an intervention other than a drug or a biological (n = 101). Eventually, 207 phase 3 RCTs met all the eligibility criteria and were selected for analysis. Included trials are listed in Additional File and their characteristics are shown in Table 1.
Fig. 1
Selection of phase 3 randomized controlled trials of pharmacological interventions used for systemic treatment of gastric cancer. 1Including trials with status ‘withdrawn’ or ‘suspended’ (n = 2), trials of pharmacological interventions administered topically (n = 1), trials concerning gastrointestinal neuroendocrine tumors (NET; n = 1), trials related to gastrointestinal stromal tumors (GIST; n = 1), and basket trials (n = 1). ICTRP International Clinical Trials Registry Platform
Table 1 Characteristics of phase 3 randomized controlled trials in gastric cancerThe investigational regimens assessed in included trials commonly involved chemotherapy (n = 90; 43.5%), and chemotherapy in a combination with immunotherapy (n = 34; 16.4%) or with a targeted drug (n = 27; 13.0%). Many RCTs (n = 84; 40.6%) evaluated the use of the investigational intervention as the first-line treatment. Most trials were conducted in the investigational sites located solely in Asia (n = 139; 67.1%). Our sample also involved many RCTs (n = 41; 19.8%) with the sites located in more than one continent. 116 (54.7%) trials had non-commercial sponsors. The largest proportion of trials (n = 88; 42.5%) comprised RCTs with the sample sizes ≥ 500.
Eligibility criteriaUpper age limitsOverall, as many as 99 trials (47.8%) had an upper age limit (Table 2). The most frequent limit, used in 56 (27.1%) RCTs, was 75 years of age. 93 (44.9%) trials listed an upper age limit of 85 years or lower (coprimary outcome). Multivariable logistic regression (Table 3) showed that the odds of an upper age limit of 85 years or lower were higher in RCTs enrolling patients with early/locally advanced resectable GC relative to metastatic GC (aOR, 2.38; 95% CI 1.11–5.21; p = 0.02) and lower in RCTs with the sites located in North America (aOR, 0.06; 95% CI 0.01–0.26; p < 0.001). However, none of the other variables including the investigational intervention type and the sponsor type significantly affected the odds of excluding older adults (p > 0.05 for each variable; Table 3).
Table 2 Eligibility criteria in phase 3 randomized controlled trials in gastric cancerTable 3 Trials characteristics affecting the odds of the upper age limits and the eligibility criteria related to the performance status of the patientTo verify the robustness of the findings from the primary analysis, we performed three sensitivity analyses. In the first analysis, for each trial, we replaced the trial’s start date with the registration date. In the second analysis, we employed a different categorization of the sample size; rather than divide the sizes into three categories as was the case in the primary analysis (≤99; 100–499; and ≥500), we used a dichotomous division for this variable (<500 and ≥500). In the third sensitivity analysis, we assessed how the variables used in the primary analysis affect the odds of the presence of an upper age limit of 75 years or lower. All three analyses had very similar results; each of them confirmed that the odds of an upper age limit were significantly lower in the trials with at least one North America-based site (p < 0.001 for each analysis; Additional Tables 3–5, Additional File). However, they failed to confirm a statistically significant association between the GC stage and the presence of an upper age limit (p > 0.05 for each analysis; Additional Tables 3–5, Additional File). Thus, overall, the variable with the strongest association with the upper age limits is the investigational site location, especially the presence of the North America-based sites (these mostly included the sites located in the USA; detailed data not shown).
We also showed a statistically significant trend to increasing the proportion of trials with an upper age limit of 85 years or lower over time in analyses involving both the trial’s start date (average change/year 0.02; 95% CI 0.008–0.03; p = 0.003) and the registration date (average change/year 0.02; 95% CI 0.009–0.04; p = 0.001).
Moreover, we found that our sample included only 3 (1.4%) trials specifically dedicated to older patients. The lower age limit in one of these RCTs was 70 years, and two others enrolled patients aged 80 years or older. In addition, one trial (0.5%) was dedicated to unfit patients aged 18 or older. None of these four trials had an upper age limit.
Performance status of the patientThe eligibility criteria involving the performance status of the patient were used in 199 (96.1%) RCTs. Most trials (n = 138; 66.7%) allowed only for the enrollment of patients with ECOG score of 0/1. The odds of excluding individuals with ECOG score > 1 were higher in RCTs started between 2017 and 2024 compared with those begun between 2009 and 2016 (aOR, 4.49; 95% CI 2.11–9.94; p < 0.001). We also noted that none of the investigational intervention types including chemotherapy or the sponsor type had any statistically significant association with the odds of excluding individuals with ECOG score > 1 (p > 0.05 for each variable; Table 3).
These results were verified by two sensitivity analyses involving some modifications of the variables used in the primary logistic regression model. Both analyses confirmed that the odds of excluding patients with ECOG score > 1 were significantly higher in more recent trials compared with earlier RCTs (p < 0.001 for each analysis; Additional Tables 6 and 7, Additional File).
Likewise, the year-by-year analyses showed a statistically significant trend to increasing the proportion of trials excluding patients with ECOG score > 1 over time, both for the trial’s start date (average change/year 0.04; 95% CI 0.02–0.05; p < 0.001) and the registration date (average change/year 0.04; 95% CI 0.03–0.05; p < 0.001).
Eligibility criteria involving comorbiditiesFull list of the eligibility criteria involving comorbidities of different organs and systems is provided in Additional File. The most common criteria concerned liver disorders (n = 170; 82.1%). The most frequent criterion referring to liver function involved aminotransferase concentration relative to upper limit of normal (ULN; n = 105; 50.7%; median cut-off, 2.5 ULN; range, 1.5–5 ULN). The proportion of trials excluding patients with liver disorders was comparable between the recent and earlier RCTs (52.9 vs. 47.1%; p = 0.28).
Many trials (n = 168; 81.2%) excluded patients with renal impairment, frequently based on creatinine concentration relative to ULN (n = 68; 32.9%; median cut-off, 1.5 ULN; range, 1–2 ULN). We found no statistically significant difference in the proportion of trials excluding patients with renal impairment between the recent and earlier RCTs (53.6 vs. 46.4%; p = 0.40). The proportion of trials with very strict eligibility criteria concerning renal function (the cut-off for creatinine clearance 60 or creatinine level ≤ 1.0 ULN) was clearly lower among recent trials (39%) compared with earlier RCTs (61%). However, this difference fell short of statistical significance (p = 0.08). A similar result was found in an analysis performed for the trials with slightly relaxed eligibility criteria (the cut-off for creatinine clearance 45–60 or the cut-off for creatinine level 1.0–1.25 ULN)—41 vs. 59% (p = 0.056).
Other commonly used eligibility criteria concerned bone marrow function (n = 157; 75.8%). The proportion of trials excluding patients with bone marrow dysfunction was comparable between the recent and earlier RCTs (53.5 vs. 46.5%; p = 0.24).
The results of the analyses of trends in the use of the eligibility criteria concerning some comorbidities over time were verified by sensitivity analyses performed by the trial’s registration date. These had very similar results (Additional Table 8, Additional File), thus confirming the results of the primary analyses performed by the trial’s start date.
Eligibility criteria concerning brain metastasesOverall, the eligibility criteria related to brain metastases were listed in 91 (44%) RCTs. 38 trials (18.4%) excluded patients with any form of brain metastases (strict exclusion), while 53 (25.6%) RCTs excluded individuals with active, symptomatic, or untreated brain metastases (conditional exclusion). In analysis by the trial’s start date, the overall proportion of trials excluding patients with brain metastases was comparable between the recent and earlier RCTs (49.5 vs. 50.5%; p = 0.65). However, the proportion of RCTs with strict exclusion was significantly higher among earlier trials compared with recent trials (73.7 vs. 26.3%; p < 0.001). By contrast, conditional exclusion of patients with brain metastases was significantly more common in recent RCTs compared with earlier trials (66 vs. 34%; p = 0.01). Very similar results were obtained in a sensitivity analysis performed for the trial’s registration date (Table S9, Supporting Information).
Eligibility criteria related to frailtyNone of the trials (0%) had any eligibility criteria related to frailty.
Comments (0)