
Remember me
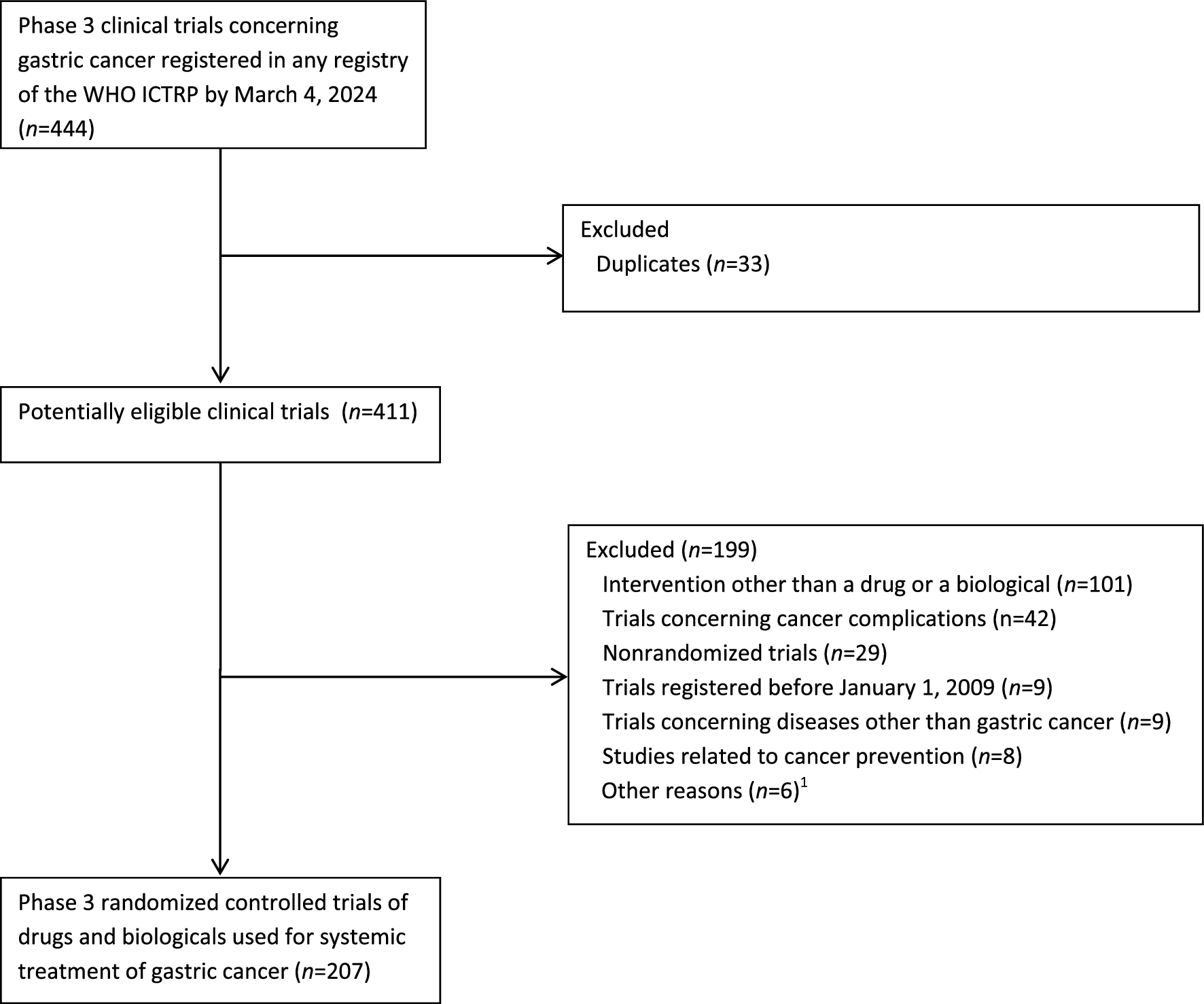

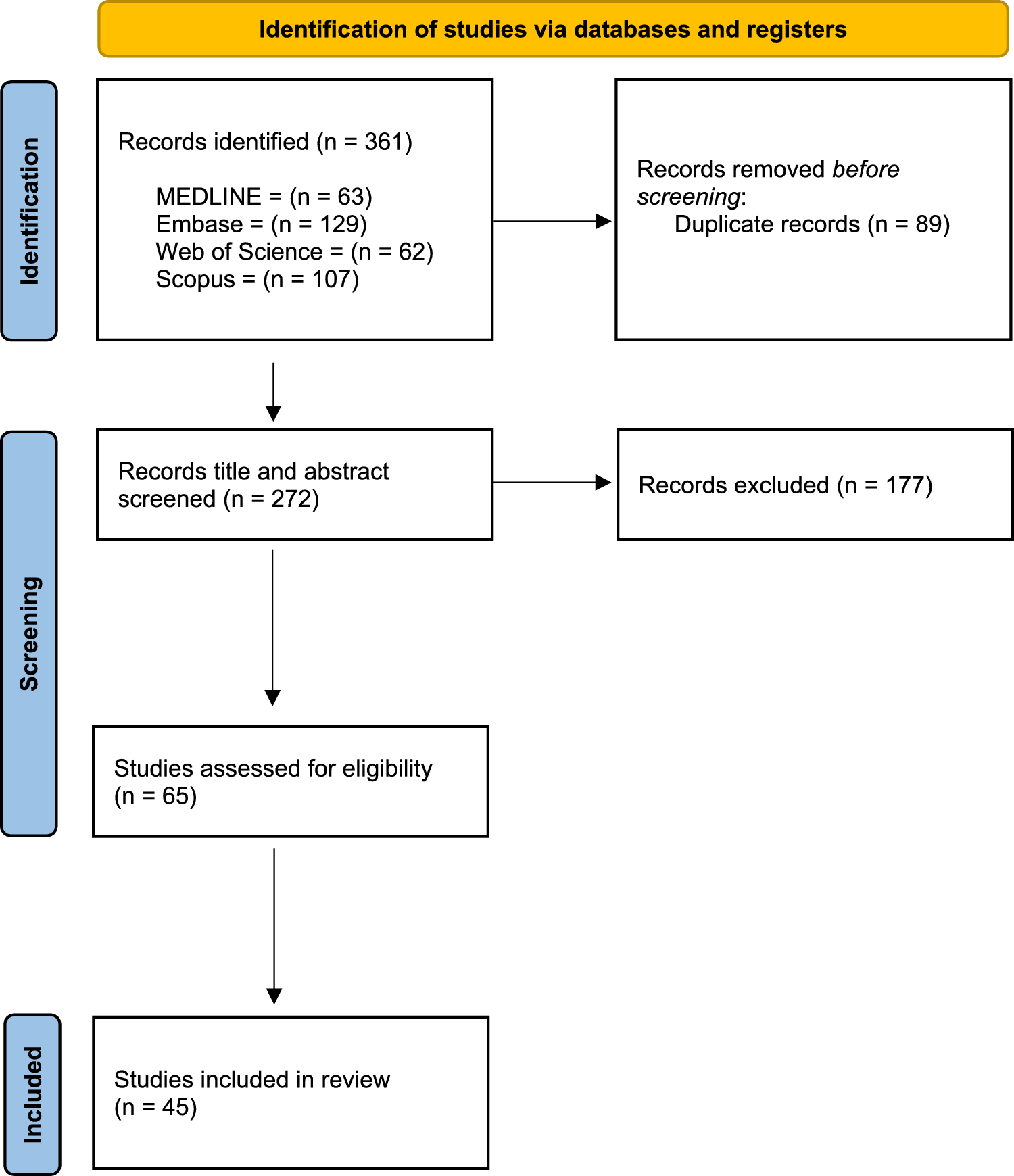
The systematic search yielded 361 records; after de-duplication, 242 unique citations remained and were screened by title and abstract. Of these, 177 were excluded, leaving 65 articles for full-text review. 45 studies met all eligibility criteria and were included in the final synthesis. The study selection process is summarised in the PRISMA flow diagram (Fig. 1). Reasons for exclusion at the full-text stage included: lack of TO/TOO reporting, or non-original, non-peer reviewed research.
Fig. 1
The PRISMA flow diagram outlining the study selection process
Study characteristicsThe 45 included studies [5, 7, 9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51] were published between 2017 and 2025 and covered a broad geographic distribution, including Europe (35%), East Asia (33%), America (24%), and Australasia (8%). Most studies were retrospective cohort or registry-based designs, with only four prospective studies and no randomised controlled trials. The majority (73%) included both total and subtotal gastrectomy. Surgical approaches were reported in 75% of studies, with open surgery reported in 20 studies, 26 reported laparoscopic gastrectomy, and 9 included robotic approaches. Several studies reported more than one surgical approach. Most studies enrolled patients with undifferentiated cancer clinical stages, although the reporting of stage distribution was heterogeneous. Study-level characteristics are summarised in Table 1.
Table 1 Characteristics of studies reporting textbook outcome and textbook oncological outcome after gastric cancer surgeryDefinitions and variabilityThere was a substantial variation in how TO and TOO were defined across the included studies. In total, 26 unique components were identified across all definitions. The most commonly used composite was that proposed by Busweiler et al. [5]; this has appeared in 9 studies. No single component was reported by all studies (Table S3). The most frequent component was the evaluation of ≥ 15 lymph nodes, which appeared in 93% of studies. Other commonly used components included no readmission within 30 days of surgery (88.8%) and a hospital stay of ≤ 21 days (88%). A detailed breakdown of component definitions and their frequency is provided in Table 2.
Table 2 Reporting frequency of textbook outcome and textbook oncological outcome criteria in gastric cancer surgeryDefinitions of TOO showed similar variability. Most studies included both pre- and postoperative guideline-concordant treatment as part of the definition. One study reported only adjuvant chemotherapy [9], whilst another did not include any systemic oncological therapy at all despite calling it TOO [10].
Achievement of textbook outcomeA total of 139,972 patients were analysed across the 45 included studies. Amongst these, 46,030 patients from 37 studies were assessed for TO, of whom 26,842 achieved TO. This represents an overall pooled achievement rate of 56%. The median TO rate was 58.6% (IQR: 37.6–75.8). In contrast, eleven studies assessed TOO, encompassing 99,568 patients, with 29,005 (29.13%) achieving TOO. The median TOO achievement rate was 30.3% (IQR: 23.6–40.2).
Components limiting TO and TOO achievementDespite heterogeneity in definitions, consistent patterns were observed in terms of which individual component most commonly limited TO and TOO achievement. Inadequate lymphadenectomy consistently emerged as the most frequent limiting factor, with studies reporting 30% compliance in some cohorts [42]. Absence of major postoperative complications was another critical determinant, with CD ≥ II being the most common barrier to TO in several studies [37, 40, 42]. In TOO-specific analyses, failure to receive guideline-concordant chemotherapy (whether neoadjuvant, adjuvant, or both) was amongst the least commonly fulfilled criteria and significantly limited TOO attainment [16]. Additionally, prolonged length of hospital stay and unplanned readmission, though less frequently highlighted, were also frequently unmet criteria, particularly when stringent thresholds (e.g. ≤ 14 or ≤ 7 days) were applied [28, 32].
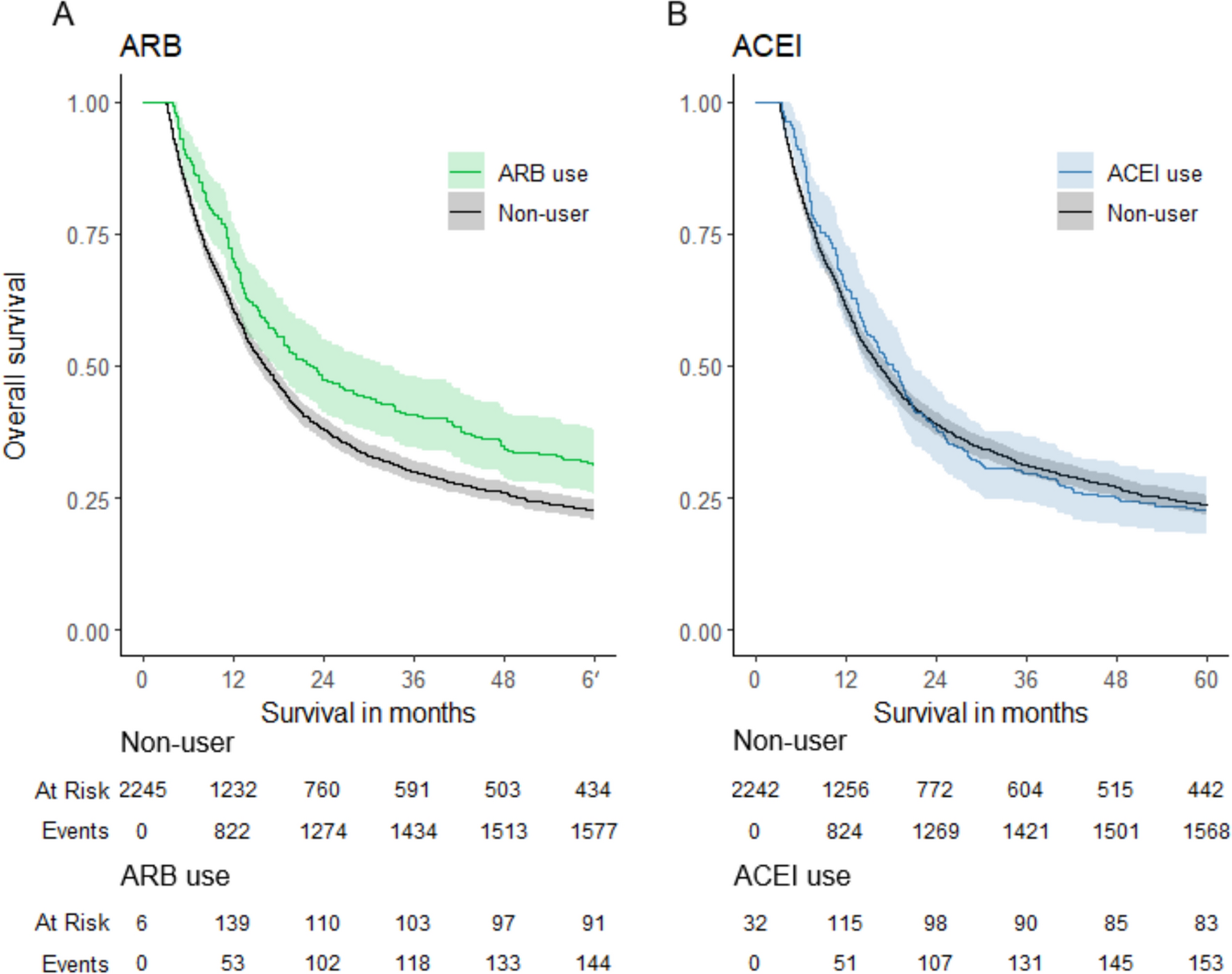
Association of textbook outcome with survival12 studies have demonstrated a significant association between achieving TO or TOO and improved overall and disease-free survival. Whilst follow-up periods varied, the survival benefit was consistently observed across 1-, 3-, and 5-year outcomes. Patients who met TO or TOO criteria had notably higher survival rates and lower hazard ratios compared to those who did not. A detailed summary of these findings is presented in Table 3.
Table 3 Survival impact of achieving a textbook (oncological) outcomeStudies analysing individual TO and TOO components demonstrate that negative resection margins (R0 resection) consistently show a survival advantage, with hazard ratios (HR) ranging from 0.62 to 0.63 (p < 0.001) [7, 28, 37, 38, 40]. Adequate lymphadenectomy (≥ 15 lymph nodes) also showed a significant association with reduced mortality in several studies [28, 37, 40]. Cibulas et al. showed a significant association with reduced risk of mortality (HR 0.79; p < 0.001) [40]. However, this association was not consistently observed across all studies, with some reporting no significant relationship [7, 35, 51]. The absence of severe postoperative complications (CD ≥ II) improves survival [7, 28, 30, 35, 38, 50, 51]: for example, patients without CD ≥ II complications had substantially better overall survival (HR 0.49, 95% CI 0.29–0.81, p = 0.006) [51]. Similarly, avoiding prolonged hospital stay (≤ 21 days) and unplanned ICU admission were independently associated with improved outcomes [37].
Patient, hospital, and treatment factors associated with textbook outcomeA range of patient-related factors have been shown to influence the likelihood of achieving TO or TOO. Reported negative predictors include older age (particularly ≥ 75 years) [7, 11, 15, 16, 28, 33, 34, 38,39,40, 42, 45], higher comorbidity burden (e.g. elevated Charlson Comorbidity Index or ASA status) [7, 9, 15, 38, 49], and adverse tumour characteristics such as larger size, higher stage [38], or proximal tumour location [28, 37]. Additional factors associated with reduced TO or TOO attainment include significant preoperative weight loss [9] and low haemoglobin [38].
Hospital-related factors play a significant role in the likelihood of achieving TO or TOO. Higher volume and surgical experience were frequently associated with improved TO rates. Studies showed that high-volume centres more often achieve composite outcomes and specific quality metrics, such as adequate lymph node retrieval [5, 43, 46, 50]. However, this association is not universally observed; for instance, the PRESTO study in Ontario did not find a significant link between hospital or surgeon volume and overall TO achievement. However, they did find that hospital volume was associated with adequate lymphadenectomy [47].
Several treatment-related factors significantly influence the likelihood of achieving TO or TOO. Minimally invasive surgery, such as laparoscopic and robotic surgery, is consistently associated with higher TO/TOO attainment, likely due to lower complication rates, adequate lymph node dissection, and shorter hospital stays [24, 42]. Some authors have considered adding MIS as a separate component of TO [27]. In contrast, open surgery and conversion from minimally invasive to open are independently linked to TO failure [33]. Whilst most sources support a positive association between MIS and TO/TOO, one study noted that laparoscopic gastrectomy favoured non-TO in their unit, potentially due to technical complexity, low case numbers, and a learning curve [21]. Subtotal gastrectomy is generally more likely to result in TO than total gastrectomy, which carries higher technical demands and complication rates [15, 28, 36]. Intraoperative factors such as prolonged operative time and increased blood loss are also associated with TO failure [25, 32]. Finally, Enhanced Recovery After Surgery (ERAS) protocols, when adhered to, improve TO rates [33], whilst compliance is influenced by surgical approach and extent of resection [15].
Comments (0)