Subtyping amyloid is a critical step in diagnosing patients with amyloidosis, as the precise identification of the precursor protein is essential for determining the appropriate treatment. For decades, the classification of amyloid subtypes has relied on a combination of clinical assessment, genetic analysis, and immunological methods [9, 18].
Table 4 Consistency assessment between Mass Spectrometry and Immunohistochemistry in amyloid subtypingMass spectrometry, by directly analyzing proteins in tissue samples, improves the accuracy of amyloid fibril characterization and is considered by some reference centers as the most reliable and the gold standard method for identifying the precursor amyloidogenic protein. Additionally, the detection of amyloid-associated proteins, which stabilize fibrils and are consistently present across all amyloid types, serves as a quality control measure, supporting the diagnosis of amyloidosis, particularly in challenging cases [10,11,12,13,14,15]. However, MS is not widely available worldwide, especially in low and middle-income countries, primarily due to its complexity, the requirement for advanced technological infrastructure, and the need of highly specialized professionals. In addition to technical challenges, financial constraints also limit the widespread clinical adoption of MS as a routine tool for amyloidosis subtyping [6, 23].
In Brazil, since the implementation of MS in 2019, the test has not been covered by health insurance. Access has been made possible through a collaborative program supported by a pharmaceutical company, thereby benefiting a larger number of patients. This is the first study to report the use of MS for amyloid typing in a Latin American country and to compares its performance with other diagnostic methods for amyloid typing.
In our study, MS proved to be a viable method for analyzing paraffin-embedded biopsy samples stored for varying periods and subjected to laser microdissection between 2.1 and 14.5 years after collection. Moreover, the technique was successfully applied to thirteen different tissue types, demonstrating its versatility. These findings reinforce the feasibility of performing proteomic analysis in non-fresh samples from various anatomical sites, allowing laboratories without local access to MS to send specimens to reference centers for amyloidosis diagnosis. Similarly, Dasari et al. reported that, among 16,175 Congo red-positive tissue samples analyzed by MS, 15,308 were formalin-fixed, paraffin-embedded biopsies [15].
Although the clinical-laboratory model correctly identified 80% of the amyloidosis subtypes, its diagnostic performance is not sufficient to justify its use in clinical practice. As an example, three cases of ATTR were initially misdiagnosed as AL, leading to one patient receiving inappropriate treatment with chemotherapeutic agents. This underscores the critical role of proteomic analysis in accurately subtyping amyloid and highlights the importance of establishing at least one reference center per region worldwide equipped with this technique.
In our study, IHC demonstrated poor diagnostic performance, correctly identifying the amyloidosis subtype in less than one-third of cases. The low positivity rate was particularly evident among patients with AL amyloidosis: the method correctly detected only 10% of cases, yielded false-negative results in nearly half, remained inconclusive in one-third, and produced false-positive results in 10%. IHC also failed to determine the subtype in approximately one-third of ATTR and AA cases. In the AFib case, the precursor protein could not be identified due to the absence of a specific antibody for this subtype in the panel.
The limited diagnostic performance of IHC observed in our cohort markedly differs from the results reported by reference centers. In a collaborative study by the Mayo Clinic and the United Kingdom’s National Amyloidosis Centre, Gilbertson et al. assessed the performance of IHC compared to MS for amyloid subtyping. By analyzing 142 biopsy specimens from 38 different tissue types, IHC correctly identified the amyloid subtype in 76% of cases, whereas proteomic analysis increased diagnostic accuracy to 94%, proving especially useful in cases with inconclusive immunohistochemical results [22]. In another real-world study, Rezk et al. demonstrated that MS identified the amyloid subtype in 80% of 320 biopsies that were inconclusive by IHC. In a subgroup with previously defined subtypes, IHC showed an accuracy of 91%. Overall, MS correctly determined the amyloid subtype in 85% of the 640 samples analyzed, underscoring its value as a complementary method when the immunological approach is inconclusive [29].
The poor performance of IHC in our study may be attributed to its known susceptibility to false-positive and false-negative results in antigen-antibody-based reactions, particularly when performed outside of specialized centers. Factors such as nonspecific background staining due to cross-reactivity with tissue proteins, or the masking of epitopes within amyloid fibrils, may lead to erroneous results. Additionally, immunohistochemical techniques rely on the availability of specific antibodies for each known amyloid subtype and do not allow for the identification of novel or rare amyloidogenic proteins. In reference laboratories, these limitations are often mitigated by the use of extended antibody panels, including both commercial and in-house antibodies, and by advanced methods such as immunogold labeling combined with immunoelectron microscopy, which enhance diagnostic precision. Unfortunately, such sophisticated techniques are not feasible in non-specialized settings. In our study, the exclusive use of commercial antibodies on long-stored tissue specimens likely contributed to the limited diagnostic performance of IHC [6, 8, 15, 19,20,21,22, 24, 25].
In middle-income countries, another important factor affecting the implementation of the most appropriate diagnostic method is cost. Considering that IHC requires a panel of multiple antibodies to cover the most common amyloid subtypes, and that MS has an average cost of USD 300, both methods may be considered cost-competitive in these settings.
In our cohort, there was a significant delay in the diagnosis of amyloidosis, highlighting the diagnostic challenges in Brazil. This is evidenced by a late diagnosis occurring approximately one year after symptom onset, often at an advanced stage of the disease and following an average of two biopsies per patient. Our findings also indicate that target-organ biopsies remain commonly used in clinical practice.
AL amyloidosis was the most frequent subtype, followed by ATTR, AA, and rarer hereditary forms such as AFib. The distribution of subtypes aligns with international data, including Ravichandran et al.‘s study of over 11,000 patients in the UK, where AL was most common (55%), followed by ATTR (21%) and AA (8%). Their data showed a decline in AA and a rise in ATTRwt over time. These changes reflect advances in treatment, greater awareness, and non-invasive diagnostic tools. In contrast, our study found fewer ATTR cases, likely due to biopsy-based inclusion criteria and evolving diagnostic practices [26].
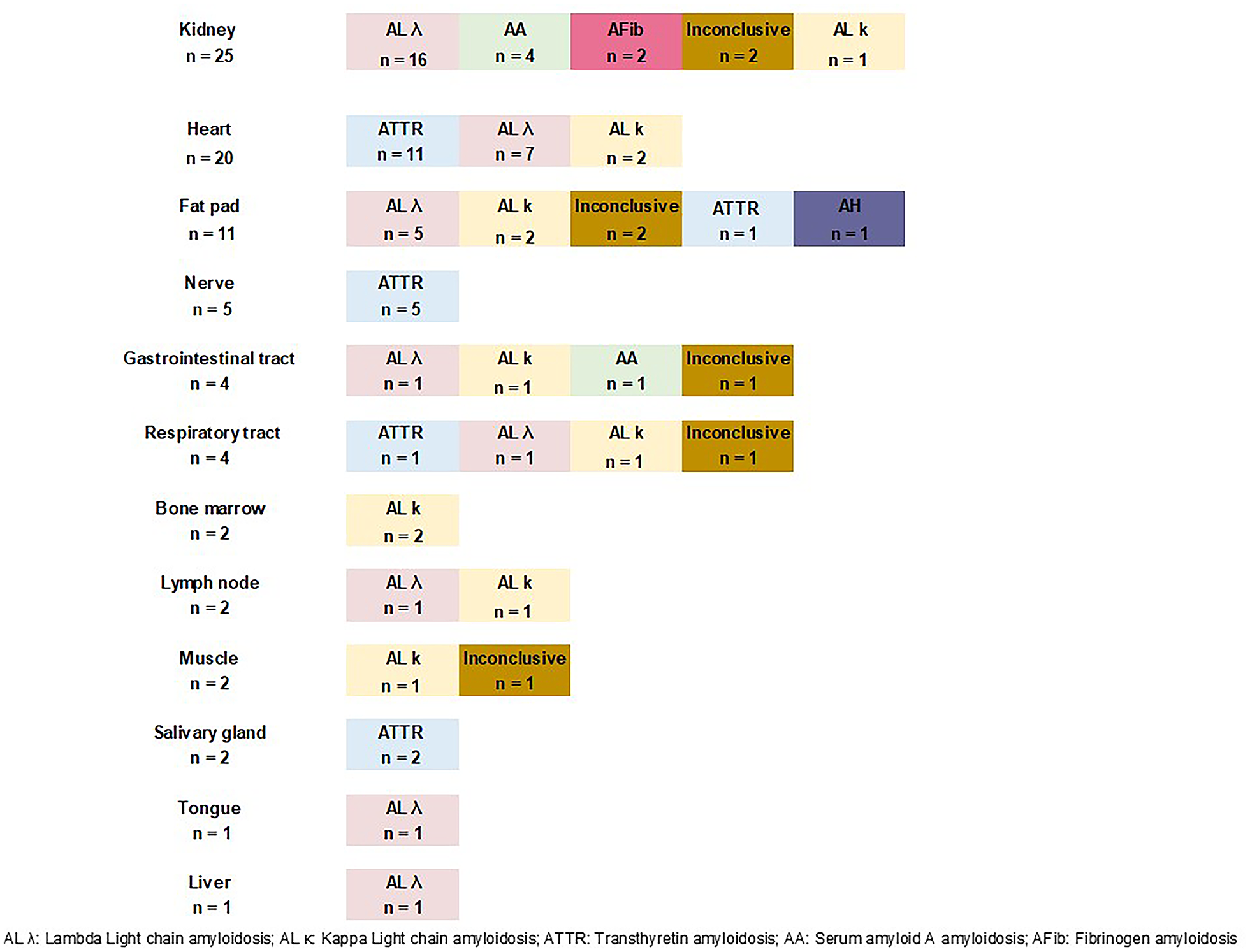
The distribution of amyloidosis subtypes reflected the organ tropism of their precursor proteins. AL amyloidosis was found in nearly all tissues, predominantly in kidneys and heart, and also in peripheral sites like fat and bone marrow. ATTR was most common in cardiac and nerve biopsies but also detected in fat, salivary gland, and respiratory tract. These findings support the use of peripheral biopsies in selected cases [1, 2, 27, 28].
As limitations of our study, the retrospective design led to the exclusion of cases due to unavailable or poor-quality paraffin-fixed biopsies, preventing MS analysis in 38% of initially identified cases. Additionally, missing clinical and laboratory data may have impacted some analyses. Another limitation was the inability of MS to determine the amyloid subtype in 9% of cases, though this did not appear to be related to sample storage duration, as it occurred in samples stored from 3.6 to 10.6 years.





Comments (0)