In an older population (average age ≥ 80 years), the initiation and continued use of a new osteoporosis drug within 3 months after a fracture prevented secondary fractures for at least 6 months after drug initiation. An effect on hip fracture prevention was observed in both sexes.
Ample evidence supports that osteoporosis medication reduces the subsequent fracture risk in placebo-controlled clinical studies in women. However, reports focusing on imminent fracture prevention are limited to RCTs [40,41,42] and real-world studies. Results from the National Registry in Sweden demonstrated that osteoporosis medication is effective in women ≥ 80 years who started treatment within 6 months after fracture; the magnitude of the effect was similar to that in RCTs [31]. The STORM cohort based on Sweden’s largest healthcare data demonstrated that anti-resorptive treatment significantly reduced hip fracture incidence and all-cause mortality in adults ≥ 75 years, though effects on any fracture were not significant [29]. A retrospective cohort study using Medicare fee-for-service also showed that osteoporosis medication continuance > 90 days decreased subsequent fractures in frail and non-frail older populations (average: 82 years), although not significantly [28]. By mimicking real clinical trials, our study demonstrates the importance of early initiation and continued use of pharmacotherapy to increase effectiveness in adults ≥ 75 years.
The influence of age on the efficacy of pharmacologic treatments for fracture risk reduction was summarized by the FNIH-ASBMR-SABRE project examining 23 RCTs in women [9], indicating that bisphosphonates reduced hip fractures with an HR of 0.47 in those aged < 70 years and 0.79 in those > 70 years; the odds ratios for vertebral fractures were 0.47–0.51 for both groups. Our results showed a similar or greater effectiveness on hip fracture with an HR of 0.60 among individuals aged > 75 years.
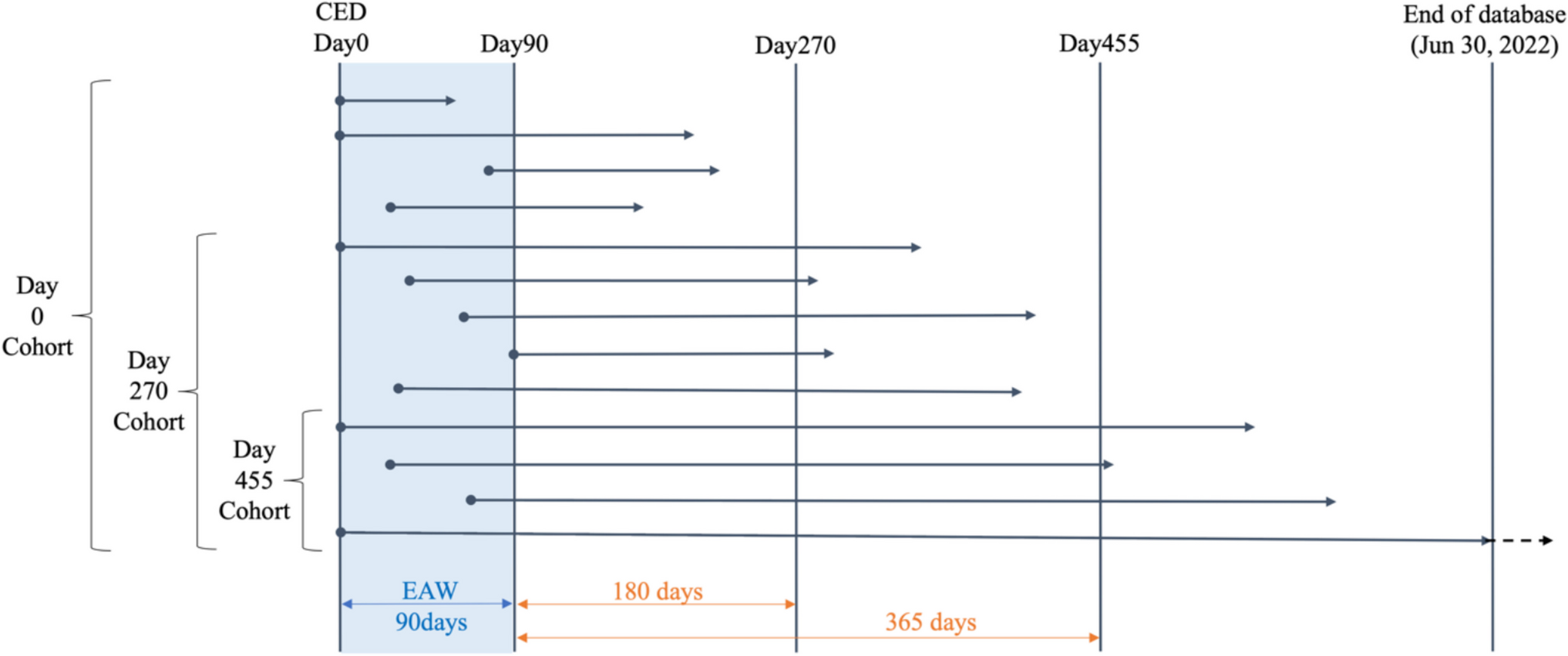
A significantly lower fracture risk in the medication group was observed for any fracture; however, site-specific analysis revealed a statistically significant effect only for hip fractures. Although a decreasing trend in the risk of vertebral, radial, and humeral fractures was noted, statistical significance was not consistently observed across all subgroups stratified by follow-up duration and sex. There are several potential interpretations of the differences in results. First, in the case of vertebral fracture, there was selection bias due to different diagnosis frequencies; the control group consisted of individuals who had never visited a medical facility or were untreated for fractures during the follow-up period. Morphological fractures diagnosed by spinal radiography may have been overlooked. Although we concluded that medication exposure had an effect, our results may have been underestimated because individuals in the treatment group regularly visited medical facilities where physicians conducted radiography and other tests, which increased the likelihood of detecting asymptomatic vertebral fractures. The control group, which did not visit healthcare facilities regularly, may have a higher likelihood of fractures that were overlooked. Second, for radius and humerus fractures, the number of incident cases was smaller compared to hip fractures. Therefore, the lack of statistical significance in the stratified subgroup analyses may be attributable to limited statistical power. Third, the length of the follow-up period may have influenced this finding. Patients in the Day 0 Cohort may have experienced a fracture before the effect of drug therapy was seen; it may have been difficult to find a difference before then, since the Day 270 or Day 455 Cohorts showed a decreasing trend, and the effect of drug exposure was more pronounced. In addition, no significant differences were observed up to 1 year (455 days) after medication initiation, but differences started to emerge after that period, suggesting that the full benefit of treatment may require sustained use for at least a year.
Osteoporosis medication can prevent fractures in women; however, real-world and RCT data on men are lacking. A recent observational study in a large integrated healthcare system compared hip fracture reduction by osteoporosis treatment between sexes [11]. The hip fracture odds ratio versus not treated was 0.26 for women and 0.21 for men (men: women = 0.81 [95% CI: 0.47 − 1.37]), indicating no significant sex effect. In the present study`s Day 0 Cohort, indicating patients who started osteoporosis treatment and continued regardless of treatment period, the HR for any fracture was 0.90 (95% CI: 0.88 − 0.94) for women, and 0.94 (95% CI: 0.90 − 1.00) for men; that for hip fracture was 0.76 (95% CI: 0.71 − 0.81) for women, and 0.81 (95% CI: 0.71 to 0.94) for men. Our results demonstrated that initiating medication within 90 days after fracture was almost equally effective in both sexes. The observed sex-neutral effect may be largely driven by hip fracture reduction. This finding is consistent with previous reports and suggest treatment efficacy is more strongly influenced by bone response than by sex [11].
In 2020, a multi-stakeholder coalition assembled by the American Society for Bone and Mineral Research recommended that the oral bisphosphonates alendronate and risedronate be first-line treatments to prevent secondary fractures among those aged ≥ 65 years with a hip or vertebral fracture [20]. Intravenous zoledronic acid and subcutaneous denosumab may be therapeutic options, and anabolic agents may be beneficial for selected patients at high risk; however, these are expensive. In our study, bisphosphonates, including a nonoral one, were used in 53.3% of patients initiating osteoporosis treatment within 90 days after fracture, teriparatide in 28.6%, denosumab in 7.8%, anti-sclerostin antibody in 5.3%, and SERM in 5.1%.
Prompt treatment is required to prevent imminent fractures. A review demonstrated a significant reduction of fracture risk after > 1 year of osteoporosis treatment for vertebral or hip fracture, while a significant reduction in the risk of non-vertebral fracture was observed after 6 months using zoledronate and denosumab in RCTs [43]. The present study found that fracture prevention is efficient at least 6 months post medication initiation. Additionally, few previous studies outside clinical trials have examined longitudinal causal relationships, but the present study demonstrated the beneficial effects of continuous medication (HR: 0.91 for Day 0 Cohort, 0.78 for Day 270 Cohort, and 0.74 for Day 455 Cohort).
We adapted the RCT design to real-world data using target trial emulation and minimized bias using cloning. Unlike previous database studies, we employed analytical methods to overcome the immortal-time bias and improve the comparability between the exposed and control participants during the observation period. Although this was not a real clinical trial, the results were devised to enhance comparative validity. However, this study had several limitations. First, the generalizability and transportability of the findings should be considered. It was difficult to distinguish detailed characteristics of the population, their living environments, and whether they were bedridden. Under the universal health insurance system in Japan, there are few disparities due to the cost of healthcare; hence, population differences do not arise in whether people receive treatment. However, these results may differ in populations in countries without universal health insurance or in situations where there are disparities in the burden of healthcare costs. Second, confounding by indication remains a potential concern. Treatment decisions are influenced by (1) unmeasured patient characteristics (e.g., disease severity), (2) physician prescribing preferences, and (3) institutional or socioeconomic factors. These factors may not be fully adjusted for, although their impact likely biases result toward the null, as more severe patients are more likely to receive treatment and experience fractures. However, selection bias could widen differences if severely ill patients avoid treatment due to personal or medical reasons. Third, the database had several limitations regarding the accurate assessment of osteoporosis and fracture outcomes. It lacked essential data such as bone mineral density, related laboratory values, unrecorded prior fractures, and information on living environments or care statuses. Additionally, the index fracture was defined as the initial fracture occurring in individuals ≥ 75 years, but prior fractures were not captured, which could affect both study groups. Claims data were used to define fracture outcomes, but this approach has inherent limitations, potentially leading to misclassification, especially for imminent fractures occurring within 180 days. To minimize such misclassification, only fractures associated with medical procedures that continued for 180 days post-fracture were considered, meaning imminent fractures within this period may have been underreported. Similarly, fractures may have been overestimated as affecting the same site due to lingering diagnoses in the medical records. Although the descriptive number of second fracture sites was a new finding in Japan, it is essential to note that caution is required when interpreting the results, given our limitations.
Additionally, differences in follow-up duration between the exposed and non-exposed groups may have influenced fracture incidence. If the exposed group had a shorter follow-up due to mortality or loss to follow-up, their fracture risk could have been underestimated. However, we adjusted for baseline imbalances, and this limitation likely led to a conservative bias. In addition, we excluded activated vitamin D (aVD) from the list of osteoporosis medications evaluated in this study, although aVD is widely used in Japan, especially among elderly patients. This decision was made to align with major international guidelines, which do not consider aVD a standard therapeutic agent for secondary fracture prevention. However, this exclusion may limit the generalizability of our findings within the Japanese clinical context. Finally, although all osteoporosis drugs were used in the same manner, each drug has a different efficacy and safety profile, and a detailed analysis of treatment patterns was not performed. The present findings reflect the preventive effects of all osteoporosis medications combined. Among the medications initiated after the initial fracture, bisphosphonates accounted for 53.3%, human anti-RANKL monoclonal antibody for 7.8%, humanized anti-sclerostin monoclonal antibody for 5.3%, SERM for 5.1%, and parathyroid hormone analogs for 28.6%. Thus, the findings of this study are likely to have been predominantly influenced by bisphosphonates. It should be noted that these results cannot be applied to evaluate the overall or site-specific effects of individual osteoporosis medications on secondary fracture.
Detailed investigations of the therapeutic efficacy and safety profile of each drug are needed. Considering the above limitations, the interpretation of the results, their applicability, and reliability must be carefully evaluated.


Comments (0)