Study cohort
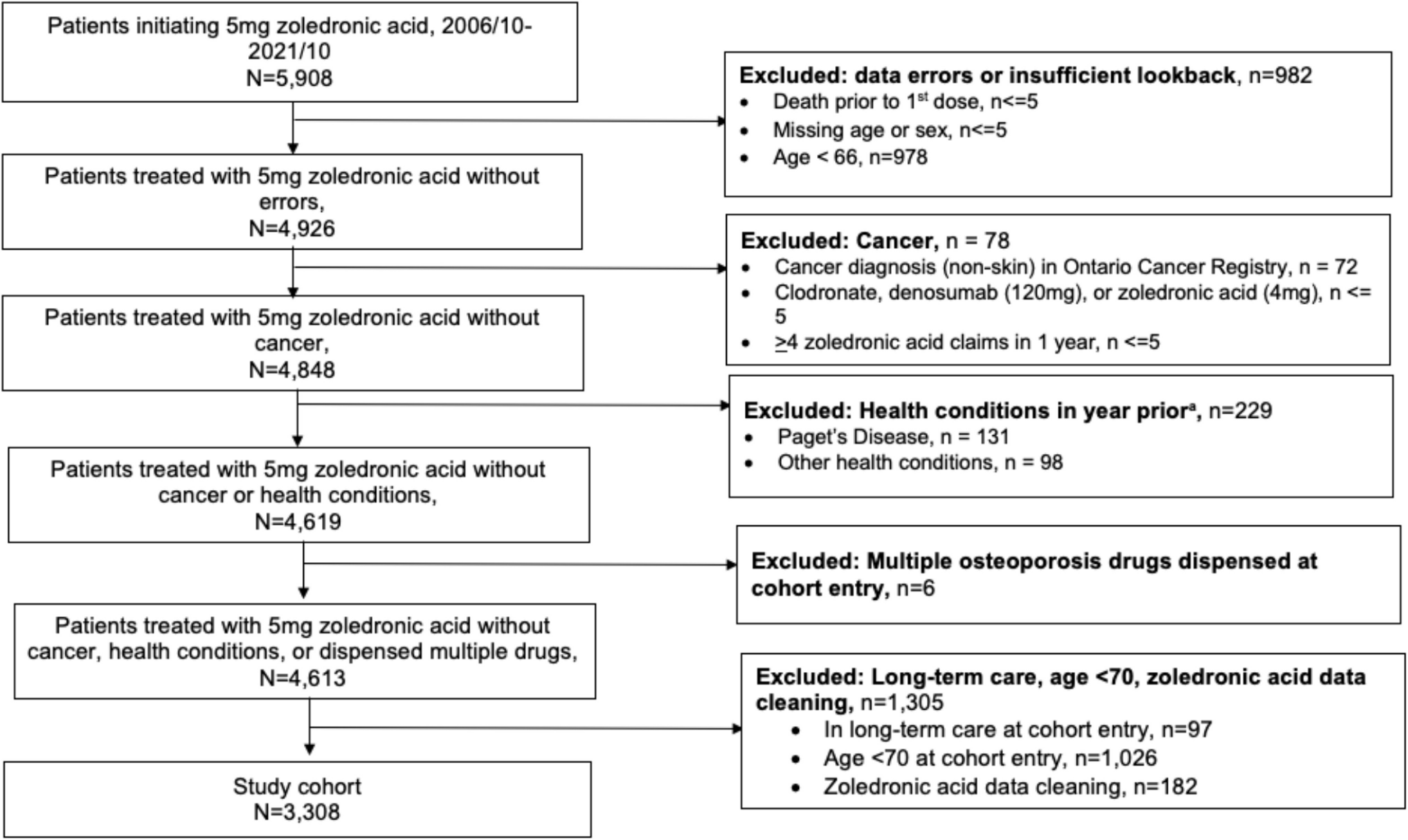
Medicare beneficiaries with Fee-For-Service (FFS) Medicare coverage between April 1, 2019, and December 31, 2021, were available. Patients were eligible if they met the following criteria: 1) initiated romosozumab treatment between April 1, 2019 (its date of initial FDA licensure), and September 30, 2020, which allowed for a minimum of 15 months of potential follow-up; 2) were women and age > = 65 years at the start of romosozumab treatment; and 3) had continuous enrollment in Medicare for at least 12 months before the initiation of romosozumab treatment. Patients with a history of Paget’s disease of bone or metastatic cancer were excluded.
Primary exposure: Social determinants of health
The county-level SES theme from the Social Vulnerability Index (SVI) was used in this study to assess community social determinants of health [16]. SVI is a tool developed to identify communities with the greatest needs during and after public health events, which is generated using 15 population-based measures from American Community Survey, including 4 different themes (socioeconomics, household composition/disability, minority/language, and house type/transportation). The SES theme is comprised based on population-based poverty, employment, income, and educational attainment measures [17]. The county-level SES theme value was assigned based on patients'county FIPS codes and then was categorized into vulnerability tertiles – low, moderate, and high vulnerability – based on the national rank [18] as the exposure factor, indicating high, medium, and low SES level respectively, with the highest tertile (lowest SES level, most vulnerable) serving as the reference category.
Outcome assessment
The primary analysis of this study focused on romosozumab discontinuation. Romosozumab discontinuation was defined as the absence of romosozumab injection records for 30 days after the previous injection (reflecting its typical dosing interval), with an additional 30-day grace period (60 days total). Patients who received 12 doses or were treated for 12 months were considered to have completed the full FDA-approved treatment course and were not eligible for discontinuation analysis. The discontinuation date was calculated as the date of the previous romosozumab injection plus 30 days. Patients were censored at the earliest of (1) death, (2) end of coverage, (3) completed 12 doses of romosozumab, (4) 12 months after romosozumab initiation, or (5) the end of the data (Dec. 31, 2021).
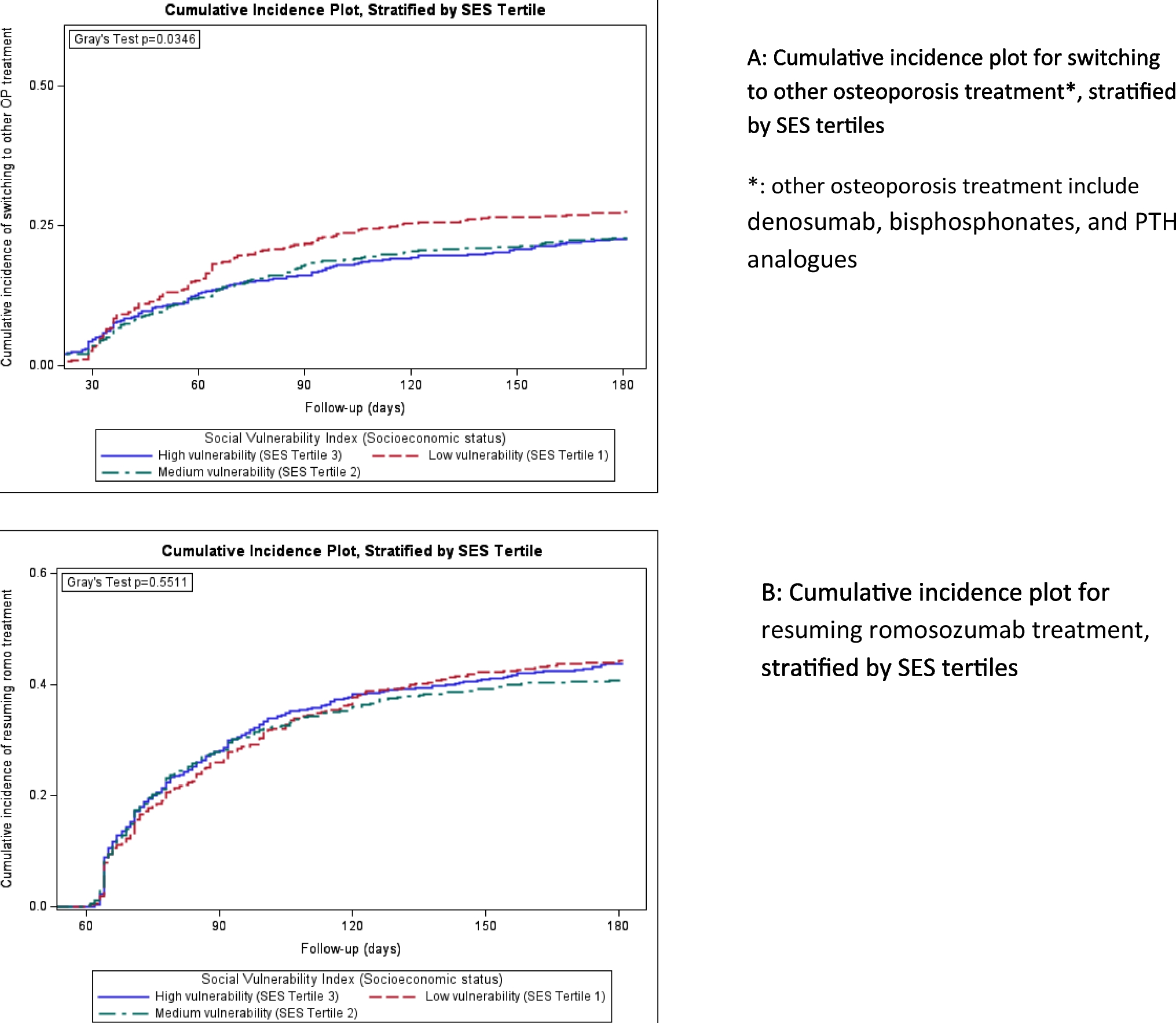
The secondary analysis of this study focused on the treatment after patients discontinued romosozumab. Osteoporosis treatments after romosozumab initiation were identified, including bisphosphonates, parathyroid hormone (PTH) analogues (teriparatide and abaloparatide), denosumab, and romosozumab re-initiation. Among patients who met the discontinuation criteria, osteoporosis treatments within 6 months after the last romosozumab injection prior to the discontinuation were examined. For the secondary analysis, treatment restart was defined as either a switch to an alternative osteoporosis therapy (bisphosphonates, PTH analogues, or denosumab) or the resumption of romosozumab within 6 months following discontinuation. Patients were censored at the earliest of (1) death, (2) end of coverage, (3) 180 days after last romosozumab injection prior to the discontinuation, or (4) the end of the data (Dec. 31, 2021).
Covariables
Based on previous studies [19,20,21,22], we identified multiple covariables, including specialty of the provider administering romosozumab, patient demographics (age, gender, race), geographic region, comorbidities, Charlson comorbidity score, medications, and healthcare resource utilization (dual X-ray absorptiometry (DXA) scan, outpatient visits, hospitalization, and emergency room visits). Medications as systemic glucocorticoid use, anti-depressant use, opioid use, and healthcare resource utilization were measured in the year before treatment initiation. Other comorbidities, including hypertension, diabetes, hyperlipidemia, heart failure, chronic lung disease, chronic kidney disease, depression, obesity, history of fracture, history of falls, and all prior treatment of osteoporosis using bisphosphonates, denosumab, or parathyroid hormone analogues, etc., were assessed using all available data prior to treatment initiation. Dual eligibility of Medicaid was used as the indicator of individual socioeconomic status. RUCA (Rural–urban commuting area) categories were further defined based on the zip codes of patient residency. Romosozumab treatment duration pre-discontinuation, health care utilization during romosozumab treatment were also examined for secondary analysis.
Statistical analysisPrimary analysis
In order to avoid the risk of unmeasured confounding related to treatment initiation time (e.g., early vs. late after approval, before and after COVID-19 lockdown), all patients were divided into three subcohorts based on the date of romosozumab initiation (index date):
Period 1 subcohort (subcohort 1): Index date between April 1, 2019, and September 30, 2019.
Period 2 subcohort (subcohort 2): Index date between October 1, 2019, and March 31, 2020.
Period 3 subcohort (subcohort 3): Index date between April 1, 2020, and September 30, 2020.
Subcohort 1 represents patients who initiated romosozumab early after approval, and subcohort 3 represents patients who initiated romosozumab after the declaration of the public health emergency.
To adjust for patient characteristics, we calculated a “discontinuation risk score” (DcRS) based on covariables described above, a concept adapted from the disease risk score. The disease risk score is the prognostic analogue of the propensity score. It is derived based on the predicted risk of disease outcome, and has been widely used to control for confounding in observational studies [23, 24]. The DcRS was estimated separately in each calendar-period subcohort for the discontinuation of romosozumab using a Poisson regression model including all covariables and the SES exposure factor (full-cohort approach) [25, 26]. Covariables were selected by a stepwise approach to achieve minimum Akaike Information Criteria (AIC). The regression coefficients from this model are then multiplied by the individual covariable values, except for the exposure factor (i.e., SES vulnerability tertiles), which is set as the reference for all participants. The sum of these products yields the subject-specific DcRS [25, 26]. Calibration plots by quintiles of the DcRS and the time-dependent receiver operating characteristics (ROC) curves were used for DcRS evaluation.
The Cox proportional hazard model, restricted to patients with overlapping DcRS, was employed to assess the association between county SES and discontinuation in each calendar period subcohort. This analysis controlled for the quintile of the corresponding DcRS.
In order to test the robustness of the association, we performed sensitivity analyses including 1) using a three-way matching weight approach [27], which was calculated by multinomial logistic regression models in each subcohort, to achieve balance of individual baseline characteristics between 3 exposure groups, and 2) using a 60-day grace period (rather than 30-day grace period) for discontinuation.
Secondary analysis
In an explorative secondary analysis, we evaluated osteoporosis treatment patterns among patients who discontinued romosozumab. Osteoporosis treatments (bisphosphonates, denosumab, PTH analogues, and romosozumab) were identified within 6 months after romosozumab discontinuation. A calendar date-dependent binary indicator for pre-post lockdown, anchored at March 13, 2020 was introduced. We used proportional subdistribution hazard models to examine the relationships between SES levels, the presence of lockdown, and the study outcomes—either treatment switch or resumption of romosozumab. The model also included an interaction term between SES tertiles and the lockdown indicator to explore if the lockdown modified the effect of SES on these outcomes.
Besides the baseline covariables before romosozumab initiation mentioned above, we also examined the treatment and healthcare utilization during the period of romosozumab treatment, period such as romosozumab treatment duration before discontinuation, out-of-pocket cost of prescription drugs, use of telemedicine, etc. Based on previous literature, we selected patients demographics (age, race), specialty of romosozumab prescribing provider, Charlson comorbidity score, history of osteoporosis treatment, history of fracture, history of cardiac infarction or stroke, baseline DXA scan, dual eligible of Medicaid, and out-of-pocket prescription drug cost during romosozumab treatment in the model, with other covariables, including comorbidities before romosozumab initiation, health care utilization during romosozumab treatment period, etc., selected by a backward elimination at the significant level 0.15 [28].
All analyses were performed using SAS, version 9.4. A two-sided p < 0.05 was considered statistically significant. Standardized mean differences (SMDs) were calculated for baseline covariates, with an SMD < 0.1 considered indicative of negligible imbalance. The research was approved by UAB institutional review board.


Comments (0)