Malnutrition significantly alters pharmacokinetic and pharmacodynamic processes, particularly in vulnerable populations such as children, pregnant women and elderly individuals. These groups exhibit unique physiological states that are further complicated by nutrient deficiencies, necessitating a more cautious and individualised approach to pharmacological care.
In children, malnutrition presents substantial challenges to drug therapy owing to developmental immaturity compounded by nutrient deficits [22]. Malnourished children, particularly those with marasmus or kwashiorkor, often exhibit delayed gastric emptying, reduced bile salt secretion and impaired intestinal integrity, all of which negatively affect drug absorption to a certain extent [22, 26, 27]. Furthermore, reductions in plasma proteins such as albumin alter the binding and distribution of protein-bound drugs such as phenytoin and diazepam [28]. Hepatic metabolism, already immature in early life, is often further compromised by malnutrition, particularly through downregulation of CYP enzymes [29]. Mukherjee et al. investigated the pharmacokinetic profiles (both maximum concentration and AUC from 0 to 4 h) of isoniazid, rifampicin, ethambutol and pyrazinamide in both severely malnourished and well-nourished children following administration of both the standard and revised World Health Organization-recommended paediatric doses [30]. Their findings revealed no statistically significant differences in these pharmacokinetic parameters between the two groups. Despite these observations, dosing of isoniazid and other anti-tuberculosis medications in children continues to follow age-specific weight bands as outlined in the updated World Health Organization guidelines. According to these guidelines, all children with tuberculosis should receive combination therapy comprising rifampicin, isoniazid, pyrazinamide and ethambutol.
A study by Dayal et al. showed no significant differences in isoniazid exposure (both maximum concentration and AUC from 0 to 8 h) between underweight, stunted, wasted, or severely malnourished children and their well-nourished peers [31]. In contrast, pyrazinamide exposure was significantly lower in severely malnourished older children with a low body mass index when compared with well-nourished children of similar age. Additionally, while the maximum concentration for pyrazinamide did not differ in underweight, stunted or wasted groups, the AUC from 0 to 8 h was significantly reduced in the stunted and wasted children.
Despite these findings, the study did not establish a clear link between reduced pyrazinamide exposure and tuberculosis treatment outcomes in malnourished children. The authors emphasised that malnutrition should not be treated as a single condition, as its various forms can affect drug disposition differently. They advocated for a more nuanced and evidence-based approach to evaluating how different malnutrition types influence pharmacokinetics in children. Thus, there remains a substantial gap in knowledge regarding how these drugs are processed in severely malnourished paediatric populations. Thus, there is an urgent need for more robust studies to better understand the pharmacokinetics of these drugs in malnourished children and to ensure accurate dosing.
Renal excretion, too, may be diminished because of reduced lean body mass and renal function. Consequently, therapeutic drug monitoring becomes essential, especially for drugs with narrow therapeutic indices [32]. It is important to base dosing on weight and developmental stage, with frequent reassessment, particularly in children who are severely wasted [33]. Moreover, micronutrient deficiencies, especially zinc and vitamin A, should be corrected to support enzyme function and optimise drug response [34].
Pregnant women present another layer of complexity. Pregnancy itself induces physiological changes such as increased plasma volume, altered gastric motility, enhanced renal clearance and fluctuating hepatic metabolism [35, 36]. When coupled with malnutrition, particularly protein-energy malnutrition, these changes can dramatically affect pharmacokinetics. The increase in extracellular fluid and total body water during pregnancy leads to an expanded volume of distribution for hydrophilic drugs, often resulting in reduced plasma concentrations [37, 38]. Concurrently, maternal adipose tissue increases by approximately 4 kg, which may enlarge the volume of distribution for lipophilic drugs [37]. However, the specific impact of increased fat stores on drug disposition in pregnancy remains poorly characterised, as available data are limited.
During pregnancy, plasma protein binding of drugs is reduced because of declining levels of both albumin and α1-acid glycoprotein [37, 39]. Physiologically, albumin levels decrease progressively as gestation advances by approximately 1% at 8 weeks, 10% at 20 weeks and 13% by 32 weeks of pregnancy [37]. These reductions may be further exacerbated by certain pathophysiological conditions that lower albumin levels beyond typical pregnancy-associated changes. Reduced protein binding increases the free (unbound) fraction of drugs, particularly for those with limited clearance, thereby enhancing their distribution into tissues [38]. For some medications, this shift has significant clinical implications. For instance, drugs such as phenytoin and tacrolimus exhibit increased unbound plasma concentrations during pregnancy due to both lower albumin levels and elevated clearance rates [38, 40]. As the pharmacological activity and toxicity of these agents are closely linked to their unbound concentrations, relying solely on total plasma concentrations for dose adjustments may result in unintended drug toxicity.
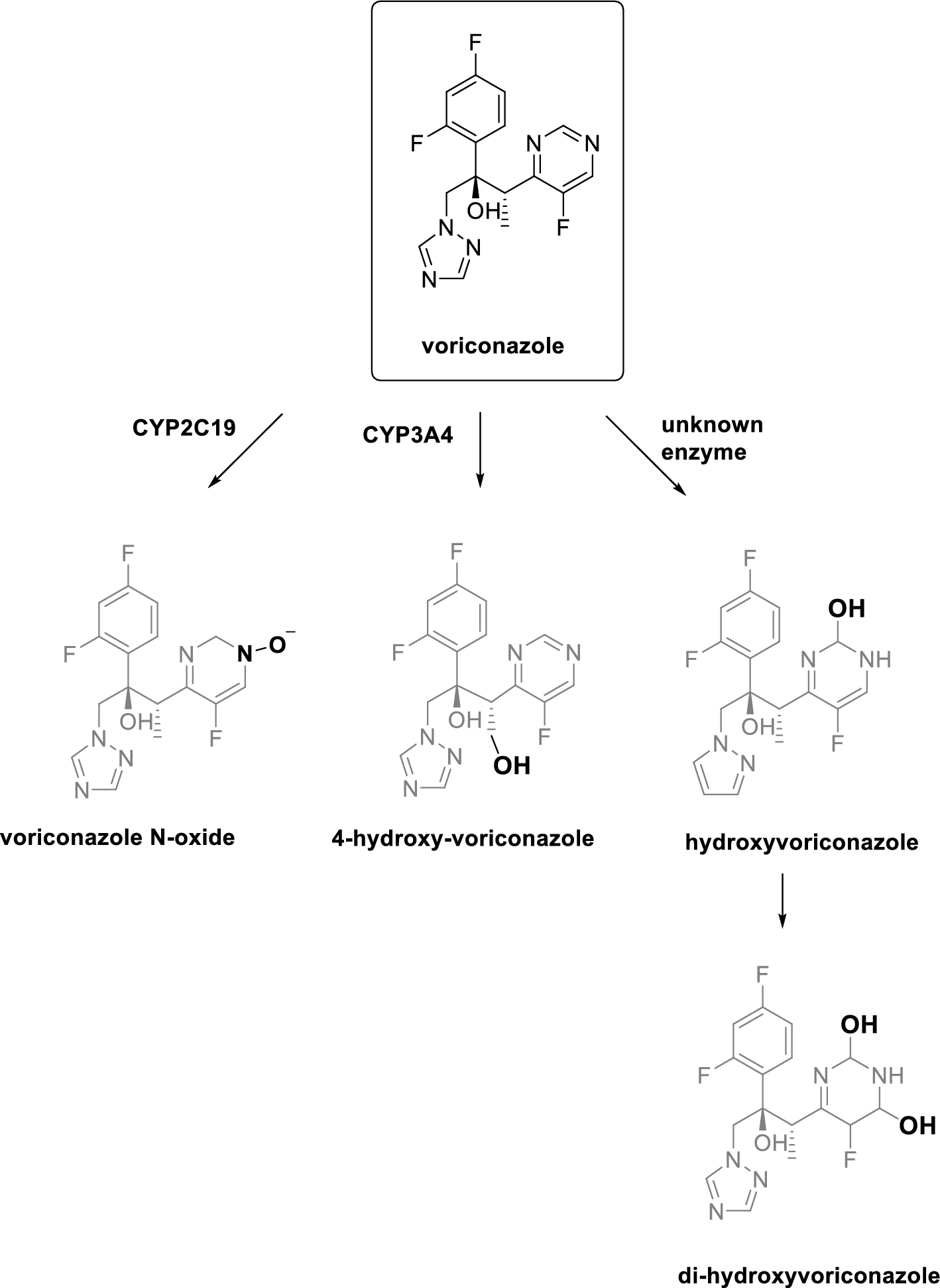
Alterations in CYP450 enzyme activity during pregnancy can significantly affect drug metabolism. For instance, enhanced CYP3A4 activity leads to the increased metabolism of drugs such as glyburide, nifedipine and indinavir. In contrast, the activity of certain other CYP isoforms, including CYP1A2 and CYP2C19, tends to decline progressively throughout gestation [36, 38, 41]. However, the clinical implications of these reductions remain uncertain and may vary depending on the specific drug involved. Therefore, a more accurate and safer approach in pregnant patients is to monitor free drug concentrations and tailor dosing accordingly, ensuring the unbound drug remains within the therapeutic window.
In Uganda, malnourished pregnant women experiencing food insecurity showed a 33% lower exposure to lopinavir compared with previously studied, well-nourished pregnant women. This reduction was attributed to decreased lopinavir bioavailability. However, increasing the dose of lopinavir/ritonavir to 600 mg/150 mg during pregnancy, using the tablet formulation, was found to restore lopinavir plasma concentrations to those typically observed in non-pregnant adults receiving the standard dose [42, 43].
Additionally, micronutrient deficiencies in pregnancy (such as folate, iron and iodine) may interfere with the efficacy and safety of prescribed drugs while simultaneously affecting foetal development [44]. Clinical care should therefore include routine nutritional assessments during antenatal visits, and where deficiencies are identified, appropriate supplementation should precede or accompany drug therapy. Drug selection and dosing should also take into account gestational age, organ function and foetal safety, using the lowest effective dose for medications with narrow therapeutic margins.
In elderly patients, age-related physiological decline is frequently magnified by malnutrition, contributing to altered pharmacokinetics and increased vulnerability to adverse drug reactions [10]. Malnutrition related to disease typically results in rapid skeletal muscle wasting, while age-associated malnutrition leads to a slower yet progressive decline in muscle mass. This protein catabolism manifests as reduced muscle mass, strength and function, significantly impairing physical performance [45]. Additionally, both malnutrition and insufficient dietary protein intake on their own have been linked to decreased bone mineral density in older adults [10, 46]. When combined with diminished physical performance and poor coordination factors that heighten the risk of falls, these changes further accelerate the development of osteoporosis and increase the likelihood of osteoporotic fractures [10]. Collectively, these consequences substantially raise the risk of falls, functional decline, loss of independence and long-term disability in elderly individuals.
Sarcopenia and a loss of adipose tissue affect the volume of distribution, altering the pharmacokinetics of both hydrophilic and lipophilic drugs [47, 48]. Malnourished elderly individuals also experience decreased renal clearance, reduced hepatic enzyme activity and hypoalbuminemia, all of which may lead to drug accumulation and toxicity [49]. Moreover, polypharmacy is highly prevalent in this group, increasing the risk of drug–drug and drug–nutrient interactions [50]. Cognitive decline, frailty and social challenges often compromise medication adherence, highlighting the need for a multidisciplinary approach [10]. Clinical strategies should include comprehensive geriatric assessments that incorporate nutritional screening, regular medication reviews, and the use of tools such as the Beers Criteria or STOPP/START guidelines to identify and minimise potentially inappropriate medications. Dose adjustments based on renal and hepatic function are crucial, as is ongoing education and support for both patients and caregivers to enhance adherence and therapeutic outcomes.
Across all populations, several cross-cutting strategies are vital to optimising pharmacological care (refer to Table 7). Individualised dosing based on nutritional status, organ function and body composition must be prioritised over standardised regimens. The integration of clinical decision-support tools can aid in identifying risks associated with specific drugs or dosing patterns in malnourished individuals. Interdisciplinary collaboration among pharmacists, clinicians, nurses and dietitians is critical to ensuring that both pharmacological and nutritional needs are met holistically. Routine screening using tools such as mid-upper arm circumference, body mass index for age or the Mini Nutritional Assessment - Short Form for elderly individuals should guide therapeutic planning [51,52,53]. Finally, patient and caregiver education is essential for promoting understanding of treatment regimens, enhancing adherence and ultimately improving health outcomes in these nutritionally vulnerable groups.
Table 7 Cross-cutting strategies for all populations

Comments (0)