
Remember me
Our systematic search retrieved 794 records: 179 from MEDLINE (PUBMED), 304 from SCOPUS, 99 from the Cochrane Central Register of Controlled Trials, and 212 from ClinicalTrials.gov. Automated tools were used in MEDLINE, SCOPUS, and Cochrane databases (English language, last 5 years), excluding 372 ineligible studies. Αn additional 52 records were marked as duplicate. Thus, 370 records (titles and abstracts) were screened. Of these, 173 were excluded for reasons such as irrelevance (n = 59), different interventions (n = 28), other cancer types (n = 34), meta-analyses/systematic reviews (n = 28), case reports (n = 1), retrospective studies (n = 1), and preclinical studies (n = 22). The remaining 197 records underwent full-text review, leading to the exclusion of 178: early-stage BC (n = 49), Phase I trials (n = 78), unspecified advanced stages (n = 8), terminated/withdrawn studies (n = 22), and no outcomes reported (n = 21). Nineteen trials met the inclusion criteria for final analysis. The steps of this screening process are portrayed in the following PRISMA 2020 flow diagram (Fig. 1).
Fig. 1
Flow diagram of search strategy according to PRISMA 2020 guidelines
Of the 19 eligible trials, 10 were Phase I/II, 9 were Phase II, and none were Phase III. Most (90%, 17/19) were open-label, with 57% (11/19) using single-group allocation and only 5 being randomized. Nine studies focused on advanced or MBC, 8 on HER2 + MBC, and 2 on metastatic TNBC. Table 1 summarizes trial categories and primary efficacy endpoints. Regarding cancer vaccine types, 6 trials evaluated dendritic cell-based vaccines, 5 peptide-based, 4 whole cell-based, 3 viral vector-based, and 1 carbohydrate-based.
Table 1 Overview of clinical trials includedPhase I/II clinical trials with cancer vaccines in advanced/metastatic breast cancerPeptide-based BC vaccinesAmong the 19 eligible trials, Phase I/II studies of peptide vaccines were common (21%, 4/19), all involving HER2 + BC and none as monotherapy. Main characteristics are presented in Table 2. Two studies, Stanton et al., and Disis et al., evaluated the HER2/neu peptide vaccine in open-label, single-group designs with approximately 20 patients each [15, 16]. In Disis et al., the vaccine was combined with trastuzumab, while Stanton et al. added cyclophosphamide, sargramostim, and HER2-specific T cells. Both had toxicity as the primary endpoint, with Disis also measuring immune response using ELISpot and HLA-A2 analysis, showing significant T cell activation in > 70% of patients. OS in Disis showed almost 50% survival at 5 years. Stanton reported immunological endpoints with 60% response and one evaluable patient showing a complete PET response [17].
Table 2 Phase I/II clinical trial data extraction categorized by vaccine typeNCT00952692 followed the same design and assessed HER2 + AS15 combined with lapatinib in 12 patients. Safety was confirmed, but only 8.3% showed a T cell response, with no Complete Response (CR), Partial Response (PR) observed.
NCT01922921 was a double-blind, randomized trial (n = 31). Both arms (1:1) received HER2 ICD peptide-based vaccines plus trastuzumab ± pertuzumab. The experimental arm also received polysaccharide-K, showing higher IFN-gamma and CD107a responses compared to the control. OS and PFS were not reported.
Whole cell-based breast cancer vaccinesWiseman et al., conducted an open-label, single-arm, multicenter trial on advanced, treatment-resistant MBC [18]. The intervention involved SV-BR-1-GM, with low-dose cyclophosphamide before vaccination and interferon alpha afterward. Tumor response (CR, PR, SD) was assessed using Response Evaluation Criteria in Solid Tumors (RECIST) and immune-related RECIST (iRECIST) criteria, along with PFS, immune response and quality of life. Among 26 patients, 23 received one cycle, 21 completed two, and 17 completed three. No Objective Response Rate (ORR), defined as CR or PR was observed, but 16.7% achieved Stable Disease (SD), with a median response duration of 105.5 days (95% CI 79–197).
Dendritic cell-based breast cancer vaccinesFour trials assessed the safety and efficacy of dendritic cell (DC)-based vaccines in BC. Soliman et al., conducted a single-center, open-label study of adenovirus-p53-transduced DC (Ad.p53-DC) vaccine plus 1-methyl-D-tryptophan (1-MT) in ER + / − , HER2 − MBC patients with p53 overexpression [19]. Of 44 patients enrolled, 39 received at least one vaccine dose. In Phase II, 19% achieved SD, while 47% had Clinical Response (CR, PR, or SD). Median PFS and OS were 13.3 (95% CI 12.97–21.85) weeks and 20.7 weeks 95% CI 25.75–46.15), respectively. Nine patients who responded to salvage chemotherapy post-trial had a median OS of 69.4 weeks (95% CI 30.1–122.1).
NCT00082641 was a randomized trial evaluating p53-infected autologous DCs in women with Stage III BC. Participants received either neoadjuvant or adjuvant chemotherapy and adjuvant radiotherapy. Vaccination schedules differed between two arms. Immune response reached 100% in the first arm and 53% in the second, indicating schedule-dependent immunogenicity.
Zhang et al., studied WT1 peptide-pulsed DC vaccines in 10 patients with advanced BC, ovarian, or gastric cancer [20]. The WT1 gene encodes a zinc finger transcription factor that is overexpressed in numerous hematological malignancies and solid tumors [21]. Among the 4 BC patients, all achieved SD after initial treatment. After completing WT1-pulsed DC vaccination, 2 patients achieved PR, while 2 maintained SD.
NCT02018458 is a parallel assignment nonrandomized trial, combined cyclin B1/WT1/CEF antigen-loaded DC vaccination with preoperative chemotherapy. Of 10 eligible patients, only those with locally advanced TNBC enrolled. The study reported 40% pathological Clinical Response (pCR) and Disease Free Survival (DFS) of 15.6 months (95% CI 6.5–26.3). No ER + /HER2 − patients were enrolled.
Viral vector-based breast cancer vaccinesNCT00088413 evaluated the clinical response of PANVAC-V (priming) and PANVAC-F (boosting) vaccines in 51 patients, including 12 with advanced BC. The vaccines target Carcinoembryonic Antigen (CEA) and Mucin 1 (MUC-1), proteins commonly overexpressed in adenocarcinomas, and were combined with sargramostim (GM-CSF) to enhance immune response without significant toxicity [22, 23]. This open-label, nonrandomized trial included three experimental cohorts. Patients received PANVAC-V on day 1, followed by three PANVAC-F doses and sargramostim at the injection site for 4 days after each vaccination. Responders could receive monthly or quarterly boosts if stable. Clinical response, assessed by RECIST over 6 months, showed that one patient (8.3%) achieved CR, four (33.3%) had SD, and seven (58.3%) experienced PD.
Phase II clinical trials with cancer vaccines in advanced/metastatic breast cancerPeptide-based breast cancer vaccinesPeptide-based vaccines offer a promising approach for advanced cancers but their therapeutic efficacy remains unproven in clinical settings and insufficient for regulatory approval [24]. Toh et al., conducted a monocentric, open-label, single-arm Phase II trial with 14 patients with refractory metastatic TNBC [25]. The vaccine contained 19 peptides. The primary outcome was safety, while secondary outcomes included PFS and peptide-specific immune induction. Main characteristics are presented in Table 3. Clinical responses per RECIST showed six patients with SD and eight with PD. Median PFS was 1.5 months (95% CI 1.0–15.6) and OS was 11.5 months (95% CI 1.5–42.1). Among 10 patients who completed the trial, PFS and OS were 5.8 (95% CI 1.4–18.9) months and 24.0 months (95% CI 2.3‐not reached), respectively. Those who did not complete the study had significantly worse outcomes, with a median PFS of 0.9 months (95% CI 0.5–1.2) and OS of 1.4 months (95% CI 1.0–6.0). The differences between groups were statistically significant.
Table 3 Phase II clinical trial data extraction categorized by vaccine typeWhole cell-based breast cancer vaccinesCytokine-modified tumor cell vaccines that secrete GM-CSF can induce robust T cell-dependent immunity. Multiple clinical studies have demonstrated their single agent safety and bioactivity in cancer patients, but their therapeutic impact remains unproven probably because vaccination alone is not potent enough to induce immune responses sufficiently [13].
NCT00971737 evaluated cyclophosphamide with an allogeneic GM-CSF-secreting breast tumor vaccine, with or without trastuzumab, for HER2 negative MBC. It was an open-label, randomized trial with two arms. The control group received cyclophosphamide and the vaccine, while the experimental group also received trastuzumab. The primary endpoint was Clinical Benefit (CB) measured by PFS at six months. Of the 60 randomized patients, 33% (95% CI 17–53) in the control group and 37% (95% CI 20–56) in the experimental group achieved CB at six months, with no significant difference between arms.
Two additional trials focused on HER2 + MBC with similar single-arm, open-label designs combining trastuzumab, cyclophosphamide, and an allogeneic GM-CSF-secreting breast tumor vaccine. The Chen et al., study reported CB at six months of 55% (11/20; 95% CI 32–77%; p = 0.013) and 40% at one year [26]. Median PFS was 7 months (95% CI 4–16) and OS was 42 months (95% CI 22–70), with a five-year survival rate of 30%. In NCT00847171, a similar regimen was used, but only 7 of the 20 enrolled patients had confirmed MBC. Among these, 6 demonstrated no evidence of disease progression in a frame of 4 years, yielding a PFS rate of 85.7%.
Viral vector-based breast cancer vaccinesThe NCT03632941 trial, presented as Crosby et al., in Table 3, was an open-label, parallel assignment study with three cohorts: VRP-HER2 immunization, pembrolizumab, and a combination of both [27]. The primary endpoint was a positive T-cell response by ELISpot over five years. The VRP-HER2 arm (n = 1) achieved a 100% response rate, the pembrolizumab arm (n = 2) had a 50% response rate, and the combination arm (n = 5) showed a 60% response rate. All arms reported a 100% SD response rate, except for one participant missing data in both the VRP-HER2 and pembrolizumab groups.
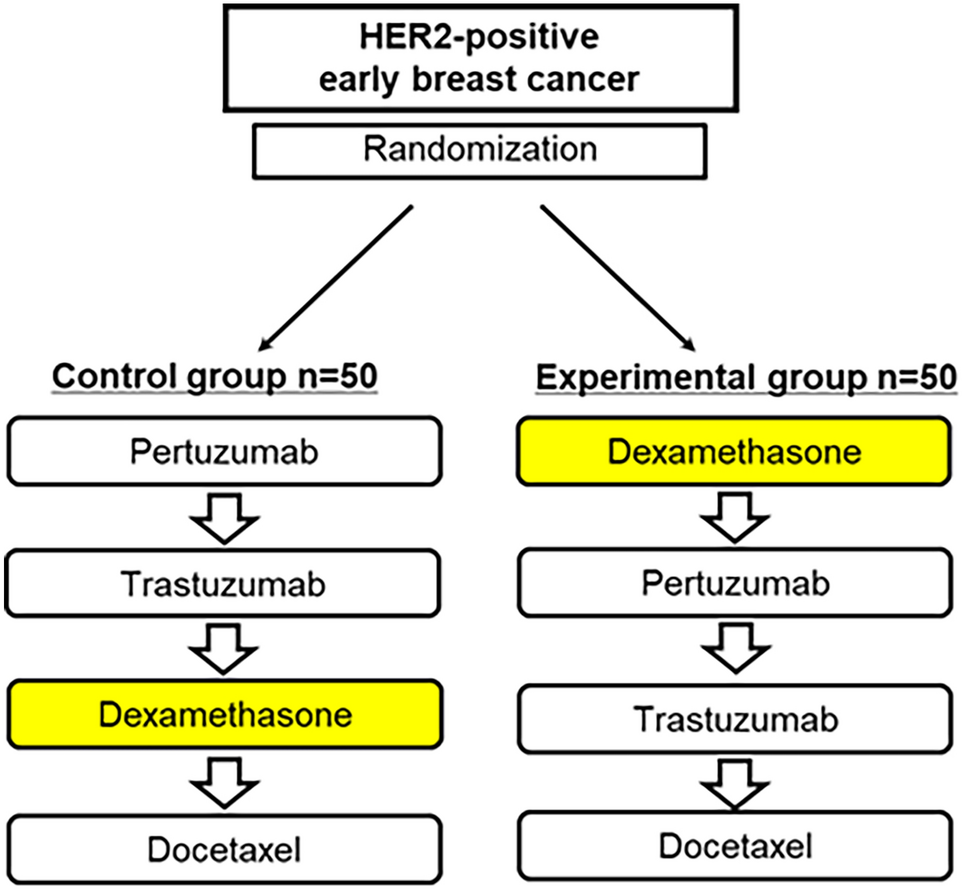
Heery et al., evaluated docetaxel with PAN-VAC in a multicenter, open-label, randomized trial. In the first arm (n = 23), patients received docetaxel and dexamethasone alone. In the second arm (n = 25), docetaxel was combined with PAN-VAC and sargramostim [28]. The median PFS was 3.8 months (95% CI 2.6–8.4) in the first arm and 6.6 months (95% CI: 3.7–9.4) in the combination arm, showing improved PFS with PAN-VAC.
Carbohydrate-based breast cancer vaccinesHuang et al., conducted a multicenter, randomized, placebo-controlled, double-blind trial enrolling 349 women with MBC who had achieved CB after at least one prior line of therapy [29]. Participants were randomized 2:1 to receive AS/OBI-821 (n = 225) or placebo (n = 124), both with cyclophosphamide. The primary endpoint was investigator-assessed PFS. Median PFS was 7.6 months (95% CI 6.5–10.9) in the AS/OBI-821 group versus 9.2 months (95% CI 7.3–11.3) in the placebo group (HR 0.96, p = 0.77). Median OS was not reached in either group. The results indicated that the disease progression occurred in 71% of patients in the experimental group and 73% of those in the placebo group. Disease progression was the primary cause of treatment discontinuation. Median OS was not reached in either treatment group by the conclusion of the trial.
Overview of clinical trial efficacy results using cancer vaccines in advanced breast cancerThe clinical results of studies included in this review are summarized in Table 4, which categorizes them based on the type of cancer vaccine. Of the 19 studies included in the review, there is significant variability in the endpoints used to assess efficacy, regardless of whether efficacy was a primary or secondary outcome. Specifically, the different endpoints reported are as follows: Number of participants with SD, Clinical Response, CB, Number of participants with Response, Number of participants with Immune Response, pCR, PFS and OS. The variability in endpoints reflects the complex nature of cancer vaccines, the diversity of BC subtypes, the stages of treatment development, and the different aims of the studies. This necessitates the use of multiple assessment methods to fully understand their efficacy.
Table 4 Summary of clinical results for cancer vaccine studies, by vaccine typeThe results were not favorable for some studies. In the study by Vincent et al., 2023, no patients responded to treatment and in NCT00088413 more than half of the patients experienced disease progression (58.3%). In addition, there are studies that showed that combining a cancer vaccine with a standard of care has no effect on its efficacy, such as in the NCT00971737 study, where the CB assessed by PFS at 6 months was 33% (95%CI 17–53) when patients received only cyclophosphamide and vaccine and 37% (95%CI 20–56) when patients received cyclophosphamide, vaccine and trastuzumab.
On the other hand, NCT00082641 showed that patients who received neoadjuvant or adjuvant chemotherapy in combination with the vaccine all exhibited an immune response, in contrast to patients who received the vaccine after adjuvant radiation therapy, where 53% of patients exhibited an immune response. In addition, there were studies, such as Heery et al. [28] Huang et al. [29] and Chen et al. [26], that reported a median PFS of approximately 7 months, with Huang et al. [29] showing the most promising PFS result of 7.6 months (95% CI 6.5–10.9) in stage IV BC. Also, in the Crosby et al. [27] study, the overall response (SD) reached 100% up to 5 years and in the Disis et al. [16] study, OS up to 5 years was 47.6%.
Although efficacy was not always the primary endpoint in the studies included in the review, most of them, 15 out of 19, focused primarily on safety or immunogenicity. In these studies, the primary endpoint was primarily the safety and toxicity of the treatment, rather than the efficacy in cancer treatment response. Most of these trials (7/8) were Phase I/II and one early Phase II as they emphasize the primary endpoints of safety and immune responses to demonstrate that the vaccine is safe and works by targeting the immune system. Efficacy is included as a secondary endpoint to examine early signs of CB, and the results presented in Table 4 are particularly promising: in the Zhang et al., [20] study, the clinical response showed 50% PR and 50% SD. In addition, in the NCT00847171 study, CB assessed by PFS was 85.7%. These findings highlight the potential efficacy of vaccines and the value of diverse endpoints in their evaluation.
Overview of clinical trial safety results using cancer vaccines in advanced breast cancerThe majority of reported Adverse Events (AEs) were only of Grade 1 or 2, data for AEs is reported descriptively in Table 5. Local complications at the injection site such as erythema or pruritus were most reported, experienced by more than half of the patients in every trial. Fever was also a commonly reported AE, while other AEs included fatigue, nausea, diarrhea, anemia or myalgia. Overall, the vaccine products were well tolerated. Most of the serious adverse events (SAEs) reported in the studies were attributed to the concomitant therapy rather than the vaccine. The AEs primarily associated with the vaccine included local reactions such as injection site reactions, extravasation changes, allergic reactions, skin infections, and urticaria. Among the 19 studies, only 3 reported patient discontinuation due to AE. In Wiseman et al. [18] 30.8% of patients enrolled in the study discontinued due to AE, with most being unrelated to the treatment except for cancer pain (probably related) and GERD (possibly related). In Vincent et al., 2023, 11.7% of patients were removed from the study due to allergic reactions (Grade 2). Finally, in Huang et al. [29] treatment discontinuation due to AEs was less than 1%. None of the 22 studies that were terminated or withdrawn were due to AE or safety concerns; the primary reasons were the lack of patient recruitment (no patients) or unavailable funding.
Table 5 Summary of safety results for cancer vaccine studies, by vaccine typeRisk of bias assessmentAmong the six randomized trials, three provided full-text results. Two of them were rated as having “some concerns” due to missing outcome data and unclear pre-specification of outcomes and analyses. One trial was judged as high risk because of substantial missing data without sufficient justification. For the remaining 13 nonrandomized and single-arm studies, two were assessed as low risk and seven as moderate risk, mainly due to limited information in protocols or registries, especially regarding selective reporting. The ROBINS-I tool was applied only to relevant domains, as certain aspects are not applicable to single-arm designs. Detailed results are presented in the Supplementary Figs. 1 and 2.
Comments (0)