
Remember me
PSMA PET imaging is now well established for evaluating biochemical recurrence (BCR) of PC, even at low PSA levels (i.e., PSA <1 ng/mL), and has also shown applications for tumor detection, primary staging, assessment of therapeutic responses, and treatment planning [2, 37, 38]. Although there are currently no universally accepted criteria for PSMA PET [39], a multidisciplinary panel of healthcare providers and PC imaging experts has recently developed a set of appropriate-use criteria for PSMA imaging [40, 41]. Utilization of PSMA PET has seen a rapid expansion in recent years, and its current clinical applications in the context of mCRPC are discussed below.
3.1 Mapping Metastatic Castration-Resistant PCPSMA PET can be highly effective in mapping the extent of disease in the mCRPC setting. In a retrospective, investigator-initiated, multicenter trial (n = 200), PSMA PET detected metastatic lesions in 56% of PSMA-positive patients (109 of 196) who were classified as non-metastatic by conventional imaging, resulting in a new treatment being initiated after PSMA PET in 62% of PSMA-positive patients (122 of 196) [42]. These patients were then followed for a median of 43 months after PSMA PET, and the associations between patient characteristics, PSMA PET findings, treatment management, and outcomes were retrospectively assessed [43]. Polymetastatic disease (defined as five or more distant lesions on PET) was independently associated with reduced overall survival (OS; hazard ratio [HR]: 1.81, 95% confidence interval [CI] 1.00–3.27; p = 0.050). Shorter time to new metastases and initial pN1 (pathological lymph node involvement) status were also associated with reduced OS, demonstrating that PSMA PET-derived disease extent allows for a more in-depth level of risk stratification in this patient population than conventional imaging [43]. The investigators concluded that the novel risk stratification approach adopted in this trial should be replicated in other studies to confirm whether these, and other risk factors for poor outcomes, could be incorporated into future treatment algorithms [43].
A multicenter retrospective study compared the prognostic value of PSMA PET staging, categorized by Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE), with established clinical nomograms in a large PC dataset [44]. Using a development cohort, two nomograms were created based on Cox regression models, assessing potential predictors for OS: a quantitative nomogram (predictors: locoregional lymph node metastases, distant metastases, tumor volume [L], and tumor mean standardized uptake value); and a visual nomogram (predictors: distant metastases and total tumor lesion count) [44]. Both were found to accurately stratify high- and low-risk groups for OS in early and late stages of PC [44]. The performance of each was then compared with established clinical risk scores, with prediction accuracy for the quantitative and visual nomograms found to be equal or superior to existing clinical risk tools [44]. An international PROMISE-PET registry study for multicenter validation of nomograms and analysis of specific patient subgroups is ongoing (NCT06320223).
3.2 PSMA PET for the Selection of Patients for PSMA-Targeted RLTPSMA PET/CT has also been carried out in people with mCRPC to confirm eligibility for RLT in clinical trials, for example, to confirm PSMA expression in metastatic sites prior to initiation of RLT in phase II/III clinical trials assessing the PSMA-directed RLT [177Lu]Lu-PSMA-617 [45,46,47] and [177Lu]Lu-PNT2002 [48].
In the open-label, randomized, phase III VISION trial (NCT03511664), the eligibility criteria included at least one PSMA-positive (tracer uptake visually greater than the liver) metastatic lesion visualized on [68Ga]Ga-PSMA-11 PET/CT. Patients with PSMA-negative (tracer uptake visually equal to or less than the liver) lesions meeting specific size criteria on diagnostic CT/MRI were excluded [46]. Patients deemed eligible by the trial-specific criteria had improved median progression-free survival (PFS; 8.7 vs 3.4 months, HR: 0.40, 99.2% CI 0.29–0.57; p < 0.001) and median OS (15.3 vs 11.3 months, HR: 0.62, 95% CI 0.52–0.74; p < 0.001) with [177Lu]Lu-PSMA-617 plus best standard of care versus best standard of care alone [46].
In the open-label, randomized, phase III PSMAfore trial (NCT04689828), the treatment eligibility of taxane-naïve patients was also determined by the presence of one or more PSMA-positive (and the absence of PSMA-exclusionary) lesions using [68Ga]Ga-PSMA-11 PET/CT [47]. The primary endpoint of median radiographic PFS (rPFS) was significantly longer in patients treated with [177Lu]Lu-PSMA-617 compared with patients treated with a change in ARPI, at 9.3 months versus 5.6 months, respectively (HR: 0.41, 95% CI 0.29–0.56; p < 0.0001) [47]. Similar to the other studies, a proportion of patients did not respond to [177Lu]Lu-PSMA-617 treatment [47].
In the TheraP open-label, randomized, phase II trial (NCT03392428), patient selection was determined by the radiotracers [68Ga]Ga-PSMA-11 and [18F]F-FDG PET/CT [45]. Significantly prolonged PSA and rPFS were observed in patients treated with [177Lu]Lu-PSMA-617 compared with cabazitaxel [45]. Of note, despite the fact that the selection used a combination of PSMA PET and [18F]F-FDG PET, a proportion of patients in the VISION and TheraP clinical trials did not respond to treatment with [177Lu]Lu-PSMA-617 [45, 46], highlighting the need to optimize methods for identifying patients who may benefit. Many oncologists may be unaware of the potential utility of FDG PET, or that it can be utilized in tandem with [68Ga]Ga-PSMA-11 to aid patient selection for treatment with [177Lu]Lu-PSMA-617, particularly in complex disease. Recent NCCN Guidelines® suggest that a combination of PSMA PET and FDG PET may be of value in mCRPC, as this combination can better detect heterogeneous PSMA expression [2]. This is particularly important, as patients with mCRPC that have metastases with PSMA-negative/FDG-positive mismatch may have poorer survival outcomes than those without PSMA-negative/FDG-positive mismatch when treated with [177Lu]Lu-PSMA-617 RLT [2, 49]. The secondary outcome study of the TheraP trial reported that the survival time of patients excluded on the basis of low PSMA expression (per PSMA PET) or discordant PET/FDG was lower than eligible participants (difference 7.8 months [95% CI 4.1–10.6; p < 0.0001]) [50]. In light of the limitations of PSMA PET in PSMA-negative mCRPC, use of additional contrast-enhanced CT or MRI is recommended for patients with PSMA-negative disease [2]. Although there is little consensus in the literature on the benefit of using FDG PET in addition to PSMA PET, in a recently conducted comparison of the trial inclusion criteria for VISION and TheraP, the investigators concluded that performing PSMA PET/CT with a contrast-enhanced CT (as performed in the VISION trial) might be sufficient for determining treatment eligibility in patients with end-stage PC [51]. Furthermore, selecting patients for treatment with [177Lu]Lu-PSMA-617 using just FDG PET alone has not been evaluated in clinical trials, as such there is a limited rationale for using FDG PET in this setting [2].
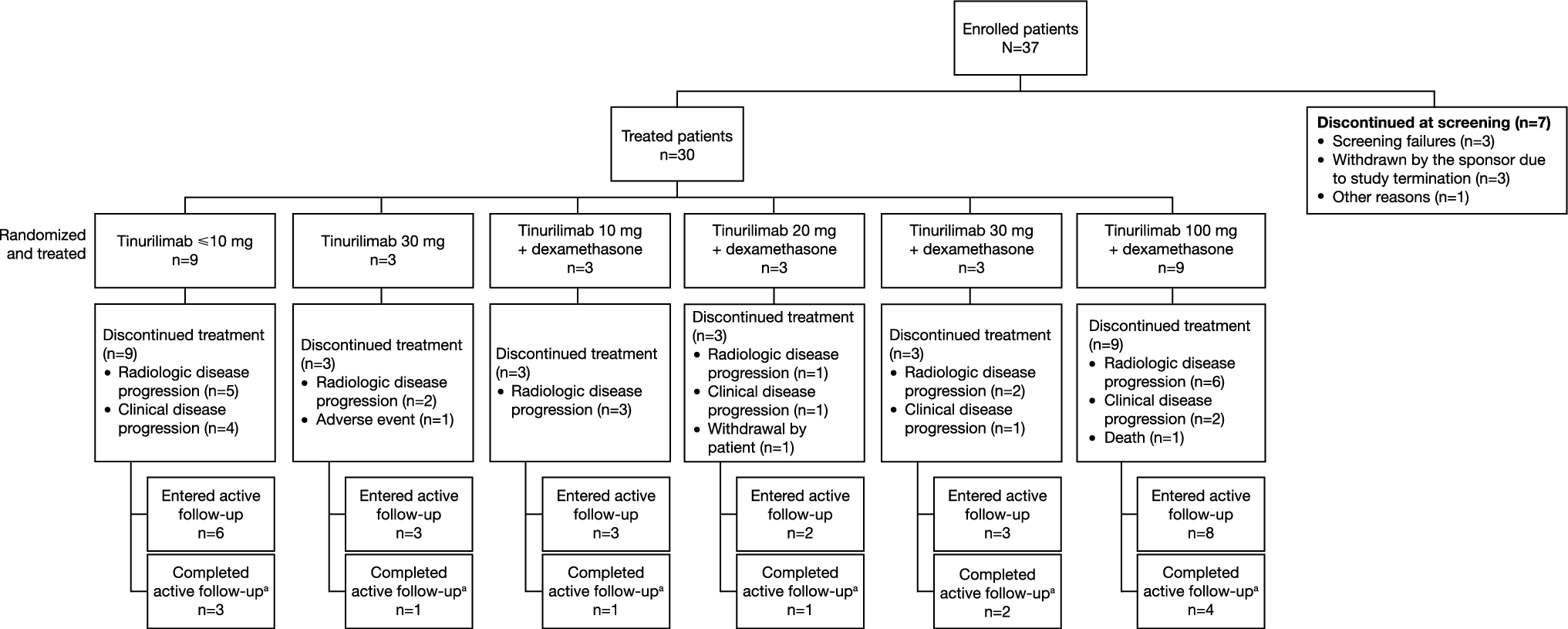
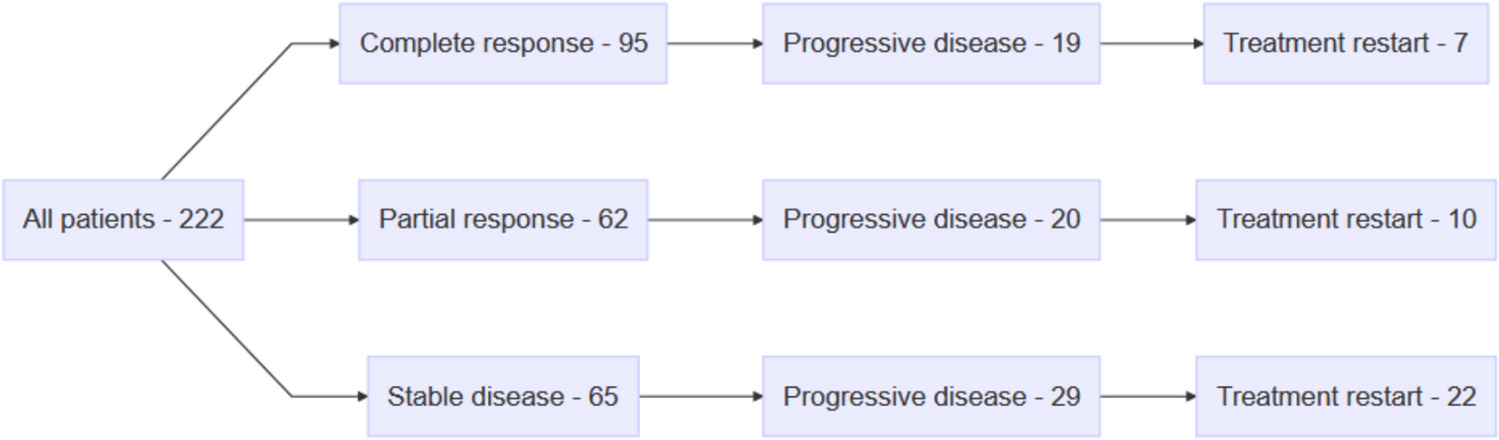
The open-label, randomized, phase III SPLASH trial (NCT04647526) is investigating the efficacy and safety of [177Lu]Lu-PNT2002 RLT versus abiraterone/enzalutamide in patients with PSMA-positive mCRPC [48, 52]. Patients eligible for a single-arm lead-in cohort study had PSMA-positive disease identified by a central reader, had one or more prior ARPI treatments, were chemotherapy naïve for mCRPC, and had adequate bone marrow and end-organ reserve [48]. A total of 27 participants met all eligibility criteria and 19/27 (70.4%) completed all four planned cycles of [177Lu]Lu-PNT2002 at 6.8 GBq (± 10%) intravenously per cycle every 8 weeks [48]. So far, preliminary data from the lead-in cohort suggest that [177Lu]Lu-PNT2002 is associated with promising dosimetry, safety, and efficacy outcomes, with a median rPFS of 11.5 months (95% CI 9.2–19.1).
As different patient selection criteria were used across these pivotal clinical trials, there is still a need for further optimization of the selection criteria for routine clinical practice, in order to ensure the maximum number of patients can derive the optimum benefit from this treatment modality. In an effort to address this issue, the Society of Nuclear Medicine and Molecular Imaging (SNMMI) released a consensus statement in 2023 recommending that treating physicians should use the phase III VISION trial criteria (Fig. 2) for selecting patients for treatment with [177Lu]Lu-PSMA-617, viewing them to be more likely to provide an OS and PFS benefit to a greater number of patients when compared with the phase II TheraP criteria [51, 53, 54]. The SNMMI group also recommended that, in addition to imaging with PSMA PET, patients should be imaged with conventional imaging (either contrast-enhanced CT or MRI) to help determine the presence of PSMA-negative disease, a particularly important consideration for patients who have known or suspected liver disease [53].
Fig. 2
© SNMMI. 177Lu lutetium-177, CT computed tomography, MIP maximum-intensity projection, MRI magnetic resonance imaging, PSMA prostate-specific membrane antigen
VISION trial patient selection criteria for [177Lu]Lu-PSMA-617 therapy for patients with metastatic castration-resistant prostate cancer. This figure was originally published in the Journal of Nuclear Medicine. Kuo PH, Benson T, Messmann R, et al. Why We Did What We Did: PSMA PET/CT Selection Criteria for the VISION Trial. J Nucl Med. 2022;63(6):816–18.
3.3 PSMA PET Interpretation and ReportingProstate-specific membrane antigen PET scan images should be reviewed and evaluated by a nuclear medicine specialist or radiologist with specific expertise [28, 55], and PSMA ligand uptake should be assessed in the prostate gland/bed, regional and distant lymph nodes, bones, lungs, liver, and other organs [12]. Clinical interpretation is typically based on a visual analysis, with the addition of quantification based on relative PSMA-ligand concentrations using standardized uptake values as an optional adjunct [12]. Furthermore, PSMA PET scan reports should provide useful findings and impressions to answer clinically relevant questions, such as patient eligibility for PSMA-directed RLT (e.g., a patient may be suitable for [177Lu]Lu-PSMA-617 treatment if their report showed alignment with the VISION trial eligibility criteria). This is an important consideration for physicians in countries where the majority of imaging is done with a combination of FDG PET and diagnostic CT, as patients in the VISION trial were deemed eligible for treatment based on PSMA PET and diagnostic CT [46, 54]. Significant differences regarding the use of [177Lu]Lu-PSMA-617 RLT in clinical practice, including assessing eligibility and treatment response, have been reported in an international study, highlighting the need for dedicated training and evidence-based recommendations as theranostics is more widely adopted [56]. The study was distributed to theranostic centers involved in patient recruitment for the TheraP and VISION trials, the corresponding authors on clinical [177Lu]Lu-PSMA-617 publications, and international contacts of the investigators; the study received responses from 95 theranostic centers (48 in Europe, 21 in the Americas, 21 in Asia, three in Oceania, and two in Africa) [56]. While there is no widely agreed consensus on the standardized reporting of PSMA PET results as of yet, a number of proposed frameworks for reporting and interpretation are available [9, 57,58,59]; these are discussed in the following paragraphs.
Interpreting physicians need to be appropriately trained to read PSMA PET imaging because differences in tracer urinary excretion, presence of non-specific uptake in bone tissue, and the potential expression of PSMA in non-prostate tumor neo-vasculature, benign lesions, and inflammatory conditions may impact the interpretation of PSMA PET imaging outputs [14, 31, 60,61,62,63,64,65]. Furthermore, training is also required to correctly interpret unexpected imaging findings, such as deviations from the typical metastatic spread of PC metastases, to avoid unnecessary biopsies of non-PC lesions [14, 66, 67].
Various different frameworks have been proposed which aim to assist interpreting different PSMA PET/CT parameters [9, 57,58,59]. The PSMA-Reporting and Data System (RADS) Standardized Reporting System version 1.0 framework is a framework that can be used for the categorization of lesions outside the prostate [58]. PROMISE has been developed as a standardized framework for the evaluation of PSMA PET using a tumor, node and metastasis frame and a molecular imaging expression score (Table 2). As PROMISE scoring is relative to the reference uptake by the liver, PSMA ligands with predominantly hepatic excretion (such as [18F]F-PSMA-1007) should be scored against uptake by the spleen instead of uptake by the liver [59, 68]. E-PSMA, the EANM’s standardized reporting guidelines version 1.0 for PSMA PET, provides consensus statements for standardized reporting of PSMA PET [9] and also includes a highly detailed template for reporting PSMA PET results [9, 58, 59].
Table 2 miPSMA expression scores from Eiber et al. [59].As PSMA technology becomes more integrated into clinical practice, there is an increased need for easy-to-use, standardized PSMA PET/CT reporting templates or guidelines, to ensure the accurate exchange of information between healthcare professionals [69]. Key information should include a summary of any prior treatments, the location and extent of radiopharmaceutical uptake in the primary tumor, and any metastatic tumor(s) that may exist, whether there are any lesions without uptake, and any additional lesions found with positive uptake on PET/CT [69].
3.3.1 Assessment of Responses to TreatmentThere is a need for well-defined progression criteria that can provide clear diagnostic information for patients and clinicians in everyday clinical practice and clinical trials [70, 71]. To date, two frameworks have been developed for the assessment of response to treatment. The Response Evaluation Criteria In PSMA-imaging version 1.0 (RECIP), which was proposed to evaluate [177Lu]Lu-PSMA-617 treatment efficacy using [68Ga]Ga-PSMA-11 PET for monitoring in mCRPC, employs the appearances of new PSMA-positive lesions and changes in total PSMA-positive tumor volume to evaluate the response to treatment [71]. These changes in total tumor volume were measured using a segmentation software for whole-body tumor quantification (quantitative RECIP) [72], yet adoption of tumor segmentation software into clinical practice is unlikely to be imminent.
A retrospective analysis found good correlation between quantitative RECIP and visual RECIP (i.e., RECIP that is determined visually by nuclear medicine physicians) for response evaluation, offering a more immediate alternative for implementation [72]. In addition, a retrospective multicenter analysis demonstrated that interim PSMA PET/CT performed after two cycles of [177Lu]Lu-PSMA-617 and evaluated by RECIP was prognostic for PSA-PFS, helping to identify those patients who are likely to exhibit disease progression [73]. Thus, PSMA PET/CT by RECIP may offer a useful approach to evaluate treatment response in earlier stages of PC [73]. Furthermore, in a small retrospective single-center study of 20 patients with mCRPC patients treated with [177Lu]Lu-PSMA-617, progression at the end of treatment assessed by RECIP 1.0 was found to be prognostic for OS [74]. However, large multicenter clinical trials are necessary to confirm these findings [74].
The second framework, the PSMA PET progression criteria, includes assessments of laboratory and clinical findings, along with recommendations for biopsy or correlative imaging [70]. In addition to this, a preliminary proposal on assessing PSMA PET response/progression from the Prostate Cancer Working Group 4 was published in September 2024 [75]. An expert committee of five experienced nuclear medicine specialists conducted an independent review of all available PSMA PET/CT scans from the open-label, single group assignment, phase I/II PRINCE trial (NCT03658447) [75], which examined the safety, tolerability, and efficacy of [177Lu]Lu-PSMA-617 in combination with pembrolizumab for the treatment of mCRPC [76]. All PSMA PET/CT scans were conducted every 12 weeks, and were blinded to conventional response prior to measuring reporter agreement [75]. The investigators found that reporter agreement on PSMA PET/CT response was “substantial” and “almost perfect” for level of response and progression, respectively; investigators also found that the Prostate Cancer Working Group 4 criteria used in this analysis could detect disease progression earlier than the Prostate Cancer Working Group 3 criteria [75]. However, as only 36 patients with serial PSMA PET/CT and CT/bone scans could be analyzed, it is difficult to draw any firm conclusions and further validation work in a larger cohort is being undertaken [75].
The SNMMI group recommends that patient response to PSMA-targeted therapy should be monitored with a contrast-enhanced CT to owing to its value in identifying soft-tissue disease (especially if uptake is low on PSMA PET) [53]. The SNMMI also highlight the value of post-treatment imaging with gamma-cameras (either planar imaging or single-photon emission CT; SPECT) [53], as [177Lu]Lu simultaneously emits two imageable gamma photons [
Comments (0)