Our study constitutes one of the most extensive real-world, observational cohorts of patients who opted for an ITH drug holiday – discontinuation of anti-PD-1 therapy—outside of a clinical trial. In most clinical trials, ITH is halted after 24 months of treatment, as per protocol. Our patients were referred to ITH drug holidays in cases of longer disease control and in the absence of immune toxicities after a median of 26 months on ITH. Clear and uniform indications for discontinuing ITH in treatment guidelines are lacking [24, 36]. Over recent years, a novel outcome measure—treatment-free survival (TFS) – has come to the attention of researchers. TFS is defined as the time from ITH discontinuation to the time of subsequent systemic therapy initiation (or death), which is in concordance with our PFS3.
As shown by long-term analysis of CheckMate trials at the 36-month mark, a significant proportion of the 1077 patients who stopped ITH treatment was still alive without the need for subsequent therapy initiation, most of whom were, per se, on drug holidays because they had finished their therapy, per protocol, not because of toxicity. Specifically, 47% of those on nivolumab plus ipilimumab, 37% on nivolumab alone, and 15% on ipilimumab demonstrated this outcome. The median TFS/PFS3 was notably longer for the nivolumab plus ipilimumab group (11.1 months) than for those receiving nivolumab (4.6 months), with a difference of 6.5 months (95% CI 5.0–8.0). Similarly, TFS/PFS3 for the nivolumab plus ipilimumab group surpassed that of the ipilimumab monotherapy group, with a difference of 8.7 months (95% CI 0.8–4.1) [37]. These data were confirmed by a recent Canadian real-world evidence report. During the 36-month follow-up, patients treated with nivolumab–ipilimumab experienced a longer duration without the need for additional ITH therapy, with a mean time of 12.4 months (95% CI 8.8–16.0) after ITH discontinuation. In comparison, patients receiving nivolumab monotherapy had a mean PFS3 of 8.9 months (95% CI 4.4–13.5), and patients treated with pembrolizumab had a mean PFS3 of 11.1 months (95% CI 8.5–13.8) [38]. All these data align with the results from the KEYNOTE-001 trial in patients who discontinued pembrolizumab upon achieving CR or PR. Of these patients, 90% were still in CR after a median follow-up of 5 years. At the long-term analysis, only 9% of patients had experienced disease progression [18]. At the same time, in KEYNOTE-006, after 2 years of pembrolizumab therapy and ≥ 3 years off treatment, 76% of patients with CR or PR had ongoing response after 5 years of follow-up [39]. Of the 103 patients who initially completed the 2-year course of pembrolizumab with at least SD, 27 experienced tumor relapse. The median PFS3 in this pembrolizumab trial was 33.3 months. Individuals with SD experienced a relapse sooner than those who achieved CR or PR [39, 40], as was also the case with our patients. In general, clinical trials and our data both prove that ITH may have a prolonged effect in disease control beyond the active treatment. Of note, the rate of CRs reported in our study (42.8%) is far superior to rates observed in Checkmate 066 and 067 and KEYNOTE-006 with anti-PD-1 monotherapy or its combination with anti-cytotoxic T-lymphocyte-associated protein (CTLA)-4, where the rate of CR ranged between 14.9 and 23.6% [22, 41, 42]. Nevertheless, this is only because our study included only patients referred to elective ITH discontinuation, and this group consisted only of individuals achieving response or prolonged stabilization. Therefore, high rates of responses were an obvious and expected finding.
It has been suggested that shorter durations of anti-PD-1 treatment might be equally as effective as extended ITH lasting ≥ 2 years [43], but our results do not confirm this hypothesis. In the NCT02673970 trial by Jansen et al. [30], the duration of anti-PD-1 therapy was shorter (median 12 months) and was also effective. Moreover, a median ITH duration of 22 months resulted in outcomes comparable to ours [44]. In the trial of 1 year of anti-PD-1 treatment, after a median follow-up of 18 months from the start of a drug holiday, 22% (n = 40) of patients experienced disease progression [30]. After a median of 12 months on anti-PD-1 treatment, the median time to disease progression was 12 months (range 2–23) [30], whereas the median PFS was not reached after a median 27 months of treatment in our cohort. After a median of 12 months on anti-PD-1 therapy, the estimated 1- and 2-year PFS rates after discontinuation (PFS3) were 90% and 71%, respectively [30], whereas they were 87.3% and 76.8%, respectively, in our cohort. After 12 months of therapy, reported relapse patterns encompassed solitary non-central nervous system (CNS) progression in six patients, CNS (brain) only progression in four patients, and multifocal non-CNS progression in three patients. Among these 13 patients, nine promptly underwent successful localized treatment for the solitary site of progression. This intervention included stereotactic radiosurgery or stereotactic body radiation therapy for three patients and surgical resection of the tumor for six patients [43]. Another report from the Huntsman Cancer Institute showed that disease progressed in 25% of patients (13 cases) who received ITH for 12 months, with a median time to progression after treatment discontinuation of 3.9 months (range 0.7–30.9). After a median follow-up of 20.5 months, 75% of patients maintained a status free from disease progression in this trial [43]. Results like ours come from the data of the report on 86 cases that included patients with and without melanoma brain metastases and who achieved CR and chose to stop ITH after a median of 22 months. In this study, disease recurred in seven patients from the group, but the median duration of survival off treatment was not reached. The median off-treatment response time was 19 months for everyone and shorter for cases with brain metastases, with a median of 17 months (range 7–41). After a median follow-up of 38 months (range 9–70), seven patients (5.6%) had died, but only one (0.8%) from melanoma [44]. In the Italian report, the median treatment time was even longer, at 33 months. In this study, 128 patients halted the anti-PD-1 treatment upon achieving CR, ten patients with SD, and 35 patients made the decision independently. After a mean follow-up period of 21 months (range 1–81), only 7.8% of those who discontinued treatment in CR experienced disease progression, whereas 20.6% faced progression after discontinuation based on the patient’s choice (including two in CR, four in PR, and one in SD) [45]. After a median 33 months of therapy, respective PFS at 12 and 24 months was 97.5% and 94.1% for individuals achieving CR before ITH discontinuation, 93.9% and 82.1% for those with PR, and 80.2% and 50.1% for those with SD [45]. A strength of our report is the high number of patients receiving ITH in the first line of treatment, whereas in the NCT02673970 trial, anti-PD-1 therapy was administered as a first-line therapy in 80 (43%) patients [30]. Based on these data, we opted for treatment discontinuation after 2 years of ITH as it was expected to be a safe choice with an acceptable risk of disease progression, with the depth of response, regardless of BRAF mutational status being a predictor of a prolonged positive outcome [18,19,20,21, 46]. We believe that the prolonged effect of ITH, also off treatment, should be attributed to CD8+ memory cells, as these cells enable long-term recognition of (melanoma) antigens after initial response. In particular, the infiltration of the tumors by memory cells – CD103+CD8+ T cells during anti-PD-1 ITH – is associated with a good prognosis [2, 47, 48].
Melanoma ITH registration trials reported that, in palliative therapy, selected clinical factors may correlate with potential long-term ITH efficacy. Data from phase II and III pivotal clinical trials confirmed that patients with high programmed death ligand-1 expression and smaller tumor burdens more frequently experienced long-term clinical benefits. Nevertheless, it was also noted that a sustained response can still occur irrespective of baseline characteristics [5]. Moreover, the Italian report found a correlation between the recurrence of melanoma during drug holidays and the primary site, with mucosal melanoma as a negative factor (HR 15.57). Moreover, a reduced incidence of relapses was reported in patients with M1b disease who experienced a CR (HR 3.84) [45]. In other real-world data, disease progression during drug holidays after 1 year of ITH in a multivariable analysis was associated with factors such as younger age, a history of brain metastasis, and elevated lactate dehydrogenase levels at the time of anti-PD-1 discontinuation [43]. We and others anticipated the rise in significance of metabolic response on 18f-FDG-positron emission tomography (PET)/CT in evaluating drug holiday candidates [46].
Few studies have also described the response after ITH reinduction. The long-term follow-up of the KEYNOTE-006 study assessed the clinical outcomes of patients who received a second course of pembrolizumab after treatment discontinuation. Among the 16 who received re-treatment with pembrolizumab, the ORR was 56%, and four patients experienced CR, five experienced PR, five had SD, and two had disease progression. The 2-year PFS with pembrolizumab re-treatment (equivalent of PFS4 in our analysis) was 62.5% [40], which is higher than the 34.3% in our population. Patients with CR or PR as the BOR to the first course of pembrolizumab in KEYNOTE-006 tended to respond better to the second course than those with SD, which is consistent with our data. Despite the constraints imposed by the limited and varied published data, we are opting for treatment discontinuation after 2 years, as it seems to be a safe choice with an acceptable risk of disease progression. Re-introducing treatment can rekindle antitumor activity in a specific group of patients following a pause in their treatment. The depth of response is currently confirmed as the most reliable predictor of a prolonged positive outcome.
van Zeij et al. [49] compared survival outcomes of patients discontinuing the treatment electively or because of treatment-limiting toxicity. They reported that the PFS and OS rates were lower in patients who discontinued the treatment because of AEs (48% and 72% at 18 months, respectively) than in patients discontinuing the treatment electively: 18-month PFS was 62% and OS 91% [49]. In our study, the PFS3 was 76.8% at 24 months after ITH discontinuation.
For patients with melanoma, the de-escalation of therapy in the form of drug holidays is safe and may be offered to those whose disease responds to first-line ITH. Patients who experienced CR before a drug holiday have a high probability of a second response at re-treatment, as suggested in lung cancer trials before including KEYNOTE-010, KEYNOTE-024, and KEYNOTE-042 studies. It is not expected that a treatment break will completely decrease the risk of ITH toxicity because of the specific mode of action of checkpoint inhibitors. Late toxicities emerging after discontinuation of anti-PD-1 therapies have been described. Most importantly, most patients with melanoma who used drug holidays with no evidence of disease progression were still progression free at 24 months after discontinuation. Patients whose initial ITH duration was <24 months and those who did not have an objective response have a higher risk of progression. ITH re-challenge enables disease control after initial progression on drug holiday. Re-initiating ITH appears to be safe and shows potential for achieving disease control. Treatment breaks after the initial response may be considered in carefully clinically selected patients with disease control. In patients with a CR and who are treated for >6 months, the risk of relapse after treatment discontinuation was low. In the future, PET–CT and liquid biopsy (e.g., circulating tumor DNA), or tissue biopsy may become recommended techniques for assessing the effectiveness of ITH with ICIs before a drug holiday. The introduction of ITH using nivolumab, pembrolizumab, and ipilimumab has significantly enhanced the prognosis for individuals facing advanced melanoma. Nonetheless, these treatments place a substantial financial strain on both patients and healthcare systems, so the first financial analyses of treatment de-escalation have been conducted. Cost-effectiveness analysis suggests that tailoring treatment de-escalation based on treatment response in patients with advanced melanoma could result in significant cost savings for the healthcare system. The authors even suggested that such an approach is a potentially cost-effective treatment mode applicable across diverse resource settings. Nevertheless, it was pointed out that clinical trials should focus on generating additional evidence regarding the noninferiority of treatment breaks to support this strategy further [50].
Our study has several limitations. First, the number of patients treated with combined nivolumab and ipilimumab, which is currently the preferred first-line ITH, was relatively low. Another limitation was the availability of drug holidays in the drug reimbursement program: patients treated before a certain time point could not be referred to drug holidays, so these patients had a longer duration of ITH to comply with program regulations. Also, data from these patients were collected retrospectively.
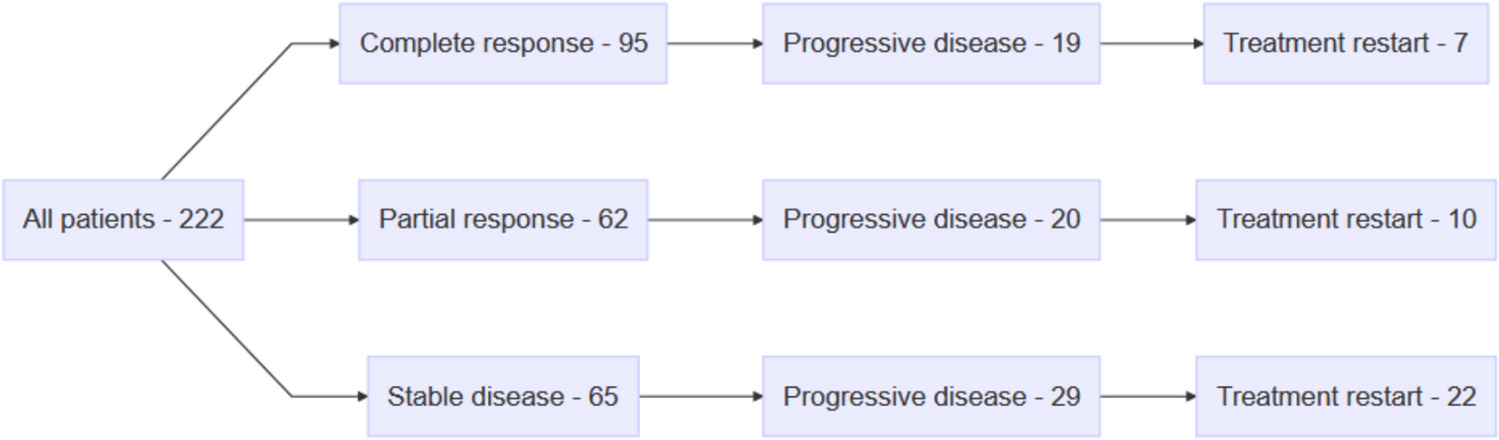
In conclusion, our study supports the elective discontinuation of ITH in patients with advanced melanoma with CR, PR, or SD. At 3 years since drug holidays were introduced, the PFS3 was 65%. In patients experiencing progression, the activity of ITH was still observed, with a 58.9% ORR to the ITH re-challenge. Patients with a CR had the most favorable survival upon ITH discontinuation, suggesting that drug holidays should primarily be considered in this group of patients.

Comments (0)