
Remember me
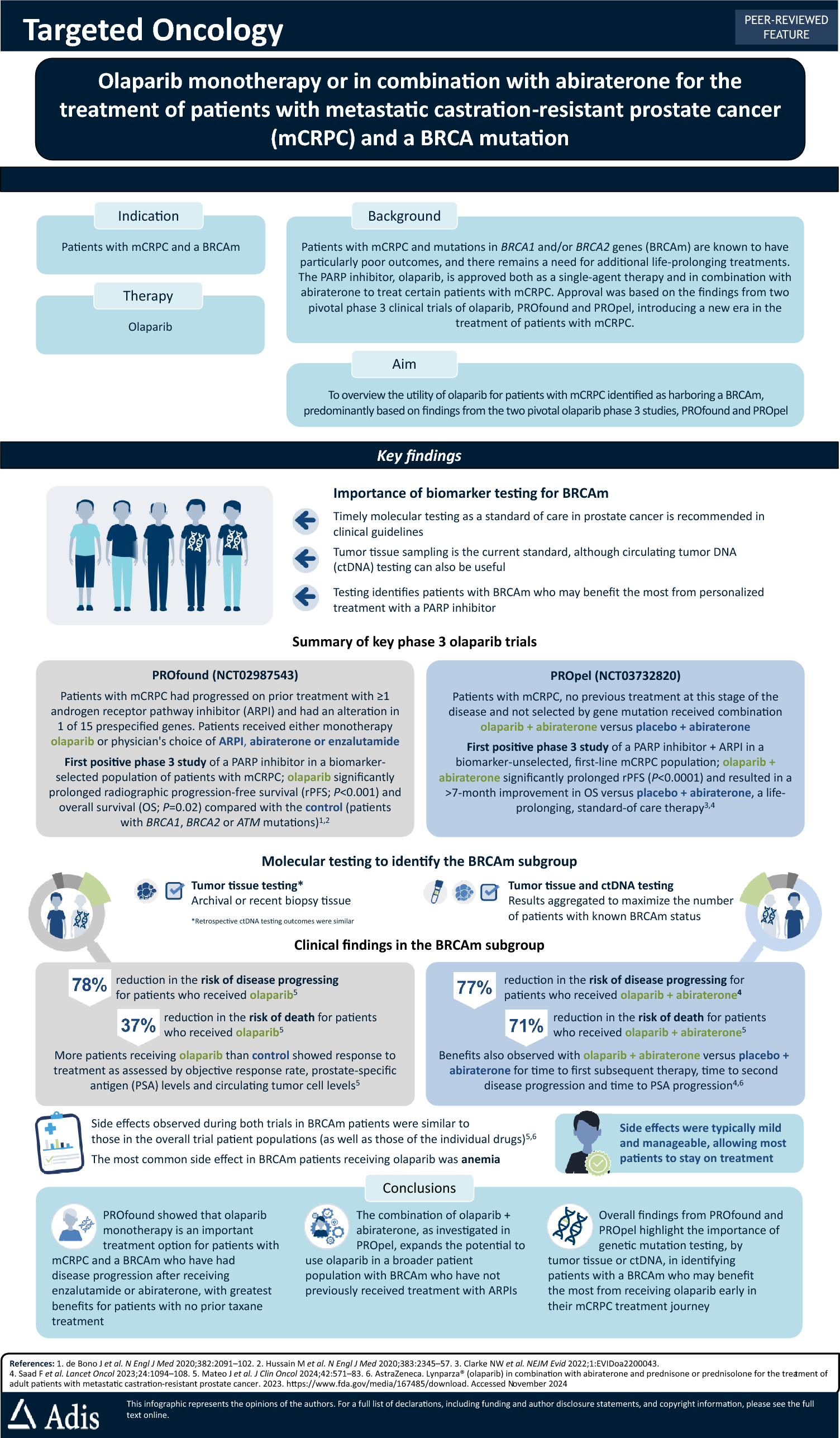
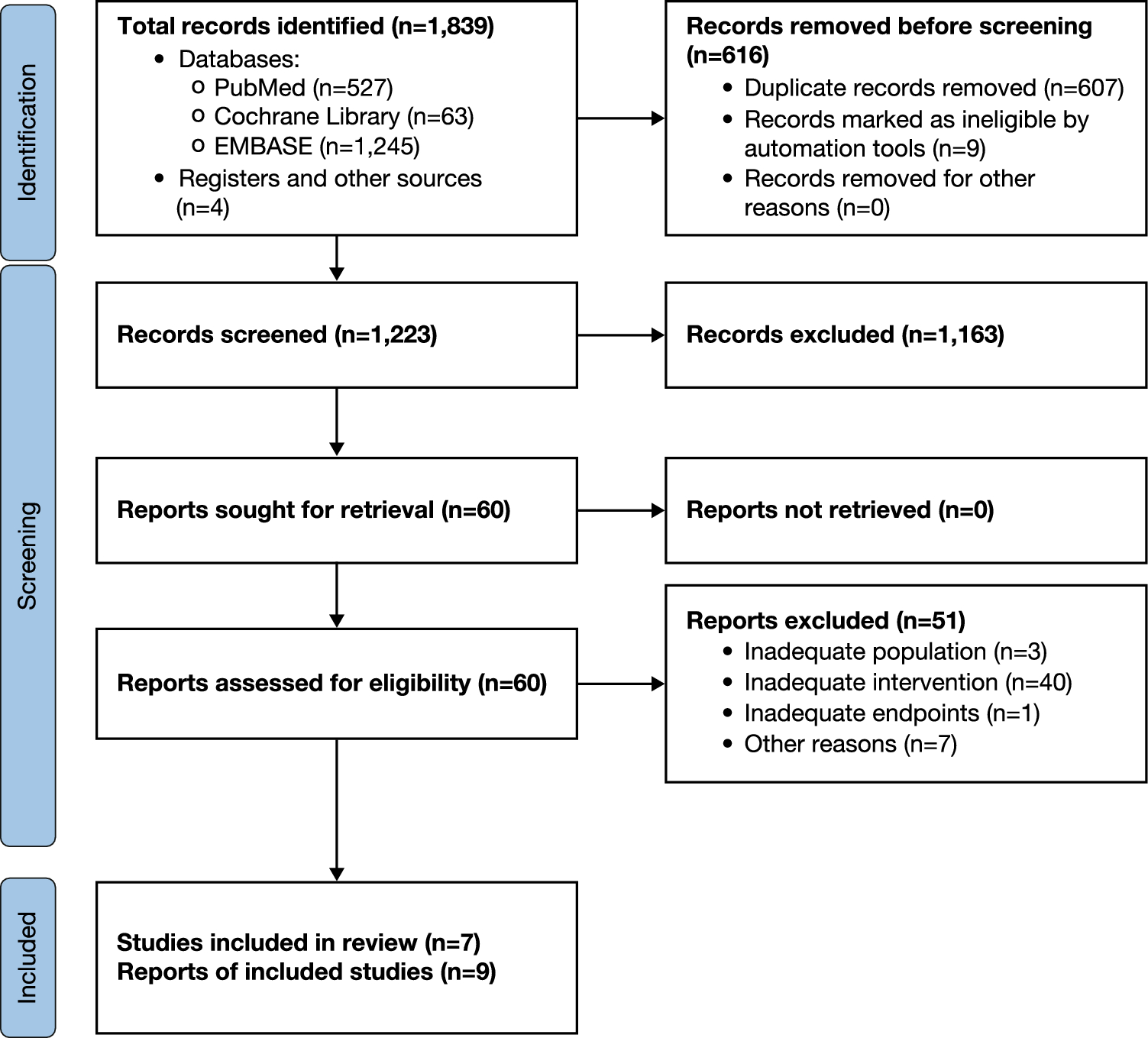
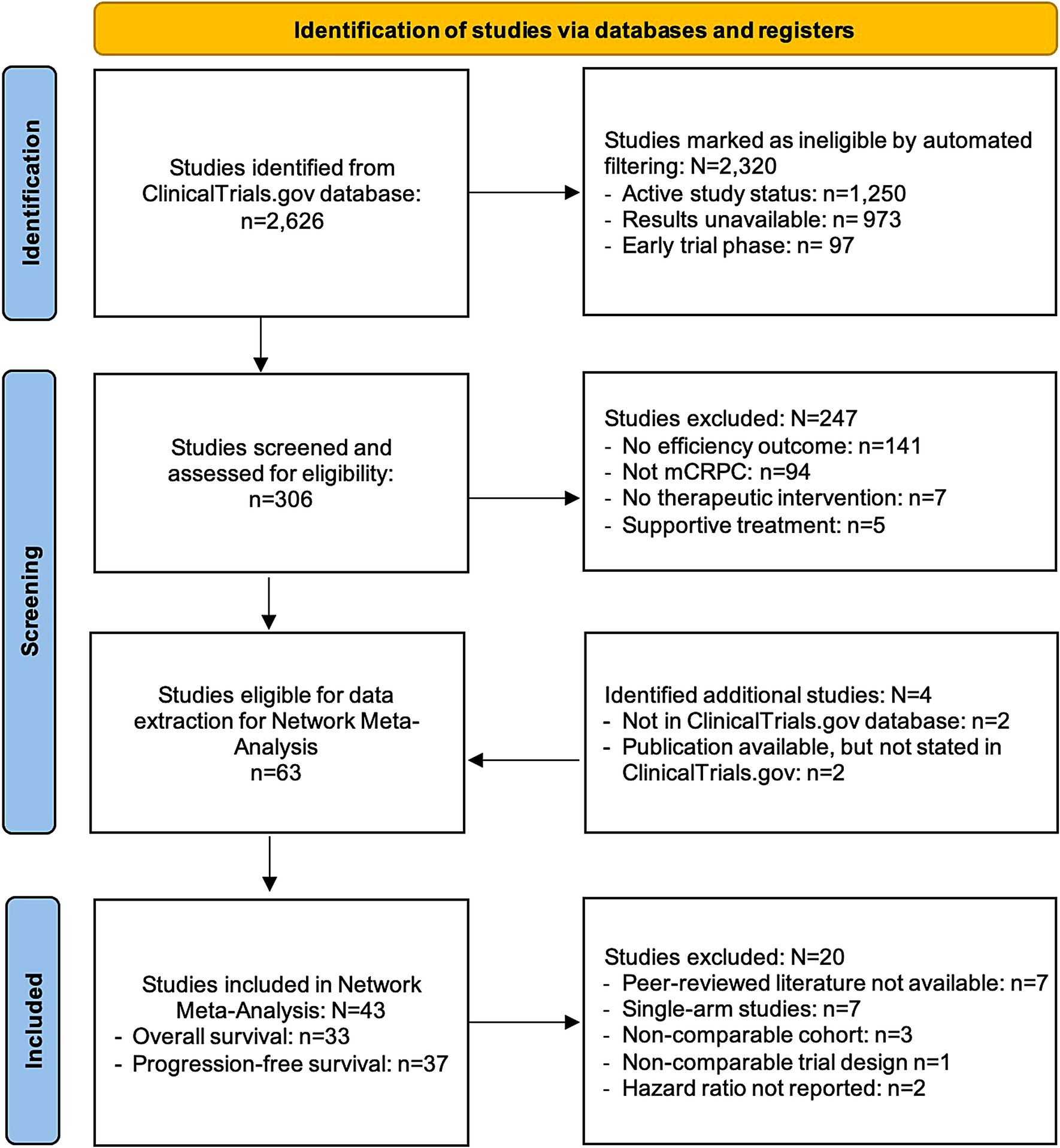
Of the 1839 potentially relevant references identified in the databases, 607 were duplicates and nine were marked as ineligible by automation tools (Fig. 1). Of the 1223 remaining records, 1163 were excluded after the initial screening of titles and abstracts. After careful review of the remaining 60 full-text articles, 51 were excluded, and seven studies described in nine publications/reports (of 442 patients treated with dinutuximab beta) were included [16, 22, 23, 25, 26, 30, 35,36,37] (Fig. 1).
Fig. 1.
PRISMA flow diagram of the literature screening process
3.2 Quality Assessment of Included StudiesAs only sparse data were available, we could not perform a reliable assessment of the risk of bias for the randomised phase of the APN311-202 study [26, 30]. The assessment of single-arm studies using the JBI Critical Appraisal Checklist for Case Series [33, 34] showed the studies were of good quality (Table S2 in the ESM), but whether participants were included consecutively in all studies was unclear.
3.3 Study DesignsThe methodology of the seven included studies is summarised in Table S3 in the ESM. Most studies were single-arm phase I and/or II interventional trials (APN311-304 [25], Flaadt et al. [16], Ladenstein et al. [35]) or observational studies (Wieczorek et al. [37], Mueller et al. [22], APN311-303 [26, 30]), and five of the studies were multicentre [16, 22, 25, 26, 35, 37]. The APN311-202 phase I/II trial consisted of two stages: a single-arm phase (stage I) [26, 30] and a randomised phase (stage II) [23, 30]. In addition, some dinutuximab beta study outcomes were compared with outcomes from historical control patients who did not receive dinutuximab beta treatment, specifically, patients from the APN311-202 and APN311-303 studies versus historical controls [26] and patients in the Mueller et al. [22] study versus a control patient population from the Associazione Italiana di Ematologia e Oncologia Pediatrica (AIEOP) database.
3.4 InterventionsAccording to the current EMA summary of product characteristics, the individual dose of dinutuximab beta is determined based on body surface area and should be a total of 100 mg/m2 per course, with each course recommended to be 35 days and a total number of 5 consecutive courses. Two schedules of dinutuximab beta administration are possible:
an LTI, defined as continuous infusion over the first 10 days of each course (a total of 240 h) at a daily dose of 10 mg/m2 [38]
a short-term infusion (STI), defined as five daily infusions of 20 mg/m2 administered over 8 h on the first 5 days of each course [38].
There were some variations in dinutuximab beta doses, infusion lengths, number of cycles, and concomitant use of IL-2 across the studies (Table S3 in the ESM).
The most common schedule was the LTI, which SIOPEN now recommends. In APN311-202, dinutuximab beta was administered as one continuous 10-day infusion at 10 mg/m2/day starting on day 8 of each cycle for a total of 5 cycles of 35–49 days, and treatment was combined with IL-2 and isotretinoin or isotretinoin alone after the dose-finding phase [26]. Mueller et al. [22] used a similar treatment regimen in which patients received dinutuximab beta at 10 mg/m2/day administered by continuous 10-day infusion starting on day 8 of each cycle for up to 6 cycles and combined with IL-2 and isotretinoin treatment. The therapeutic regimen in APN311-303 provided a continuous 10-day infusion of dinutuximab beta at an initial dose of 5 mg/m2/day in the first cycle, followed by 10 mg/m2/day in subsequent cycles, with patients receiving a total of up to 6 cycles every 28–35 days and receiving combination therapy with IL-2 and isotretinoin [26]. A recommended dose of 10 mg/m2/day of dinutuximab beta was given in APN311-304, with patients receiving a continuous 10-day infusion for up to 5 cycles of 35 days without IL-2 or isotretinoin [25]. Similarly, Wieczorek et al. [37] reported that patients received dinutuximab beta at 10 mg/m2/day by continuous 10-day infusion per 35-day cycle for up to 5 cycles and isotretinoin combination treatment with the addition of IL-2 in individual patients.
Two studies evaluated the STI schedule, which involved dinutuximab beta administered by 8-h infusion. Flaadt et al. [16] reported that patients received dinutuximab beta 20 mg/m2/day by 8-h infusion on 5 consecutive days (total 100 mg/m2/cycle) for a total of 6 cycles of 4 weeks and also received low-dose IL-2 in cycles 4–6 [16]. The dose of dinutuximab beta was established in a phase I dose-finding study using an 8-h infusion over 5 consecutive days for up to 3 cycles of three different dose levels (10, 20, or 30 mg/m2/day), although patients in this study, reported by Ladenstein et al. [35], did not receive IL-2 or isotretinoin combination therapy.
All patients received the recommended supportive treatment during the administration of dinutuximab beta, including pain management with oral gabapentin and morphine, and prophylaxis of fever with metamizole, acetaminophen, or ibuprofen, according to institutional standards [38, 39]. All patients received hydration during administration of dinutuximab beta to prevent hypotension.
3.5 Baseline Patient Demographics and Disease CharacteristicsPatient demographics and disease characteristics at baseline are summarised in Table S4 in the ESM for the included studies and the historical controls. All included studies evaluated the use of dinutuximab beta in paediatric populations with HR-NB, although the upper age limit differed between the studies, with some studies including patients aged up to 26 years. The mean age at study entry was comparable between studies (5.1–6.4 years). The majority of patients in most studies were male, although there was some variation (43.8–76.5%) between the study populations. All studies included patients who had either relapsed or refractory disease, but the proportions varied across studies (relapsed 32–95.6%; refractory 4.4–71.6%). In all studies, most patients had International Neuroblastoma Staging System (INSS) stage 4 disease (76.5–96.6%). The percentage of patients with MYCN amplification varied across studies (7.1–62.5%).
Some studies reported the number of patients with evaluable and measurable disease. The evaluation of the disease status with all recommended methods was obligatory before study entry; however, the available data were insufficient to evaluate how many patients had disease present in one examination only. In APN311-202, in patients with relapsed and refractory disease, disease evaluated by magnetic resonance imaging and/or computed tomography was present in 21.1% and 32.0% of cases, respectively; and 42.1% and 52.0% of patients had evaluable disease assessed using MIBG and/or bone marrow histology, respectively [26]. Similarly, disease in APN311-303 in patients with relapsed and refractory disease measured by magnetic resonance imaging and/or computed tomography was present in 23.3% and 40.0% of cases, respectively, and disease detected by MIBG and/or bone marrow histology, cytology, and immunohistochemistry only was present in 53.3% and 46.7%, respectively [26]. Measurable disease was recorded in 26.5% and 81.3% of patients in the studies by Flaadt et al. [16] and Ladenstein et al. [35], respectively. Evaluable disease was reported in 77% of patients in the study by Mueller et al. [22].
In all studies, disease stabilisation was required as a minimum response before immunotherapy. High-dose chemotherapy after conventional chemotherapy was one of the inclusion criteria before immunotherapy in most studies, but the type, time, and treatment line in which autologous stem cell transplant was to be performed was not strictly defined, with the exception of the Flaadt et al. [16] study, in which haploidentical stem cell transplantation was always performed directly before immunotherapy.
Prior exposure to anti-GD2 therapy was an exclusion criterion in most studies but was permitted in APN311-304 if the patients did not have human anti-chimeric antibodies (HACA) [25] and in the study by Wieczorek et al. [37].
3.6 Response to TreatmentDisease evaluation was performed immediately before immunotherapy and after cycles 2 and 5, except for in the study by Flaadt et al. [16], in which response to treatment was evaluated after cycles 3 and 6 as well as at the suspicion of disease relapse or progression. Therefore, the timing of when relapse or progression was suspected should not majorly influence any comparison of response across trials. In all studies, patients were followed up every 3 months after the end of therapy and evaluated every 3–12 months for up to 3–5 years. The International Neuroblastoma Risk Group criteria for disease evaluation [40] were used in all included studies, although response was not confirmed by independent reviewers in all studies.
Response to dinutuximab beta used in maintenance therapy was evaluated only in patients in whom it was possible to assess response before maintenance; response rates are summarised in Table 1. How response was reported varied among the studies, with some studies reporting only best response throughout the study and others reporting response rate at the end of planned therapy. Best response rate varied from 28.6% to 54.8% across studies.
Table 1 Efficacy results of included studies (in alphabetical order)In APN311-202 stage I, the ORR (complete response [15] or partial response [PR]) as the best response was 54.8%, including eight patients (25.8%) with CR and nine patients (29.0%) with PR, and at the end of study, ORR rate was 45.2% including six patients (19.4%) and eight patients (25.8%) with CR and PR, respectively [26]. In APN311-303, the ORR as the best response was 40.5%, with 13.5% of patients with CR and 27% of patients with PR, whereas the ORR at the end of the treatment was 32.4% (CR 8.1%; PR 24.3%) [26]. In APN311-304, best ORR throughout the study was 36.7% or 52.6% when including minor response; additionally, ORR at 24 weeks after the end of cycle 5 for the whole population was 26.3% or 31.6% when including minor response [25]. In Mueller et al. [22], the best response rate was 40.5%, which included 13.5% patients with CR and 27.0% patients with PR [22]. In the Wieczorek et al. [37] study, the ORR at the end of dinutuximab beta maintenance therapy in patients who had active disease before immunotherapy was 76.5%.
Response rates were higher for patients with refractory disease than for those with relapsed disease; however, not all included studies reported subgroup results. In stage I of APN311-202, response was better for patients with refractory disease (48%) than for those with relapsed disease (33%) [26], as was the case in study APN311-304, with a best response of 47.1% and 28.6%, respectively [25].
APN311-304 separately evaluated responses for patients with osteomedullary disease and soft tissue disease; the response rate was highest in patients with bone marrow involvement (93%), with a 53% response rate in patients with osteomedullary disease [25]. Even if the response was evaluated separately, the patients might have had disease in both the osteomedullary compartment and soft tissue.
3.7 SurvivalAll studies reported survival outcomes after at least 3 years of follow-up from dinutuximab beta treatment. The EFS, PFS, and OS data for patients receiving dinutuximab beta are summarised in Table 1. All studies reported OS, with the endpoint of EFS (defined as the time from randomisation or treatment initiation to recurrence or progression of disease, secondary neoplasm, or death from any cause [41]) reported for APN311-202 [26], APN311-303 [26], and Flaadt et al. [16] or the endpoint of PFS (defined as the time from randomisation or treatment initiation to relapse/recurrence or progression or death from any cause [41]) reported for APN311-304 [25], Mueller et al. [22], and Wieczorek et al. [37]. Ladenstein et al. [35] did not report EFS or PFS.
For all patients in stage I of APN311-202, the 3-year EFS and OS were 41.1% and 54.0%, respectively [30]. In the randomised group (stage II) of APN311-202, survival outcomes were comparable in patients receiving dinutuximab beta alone or combined with IL-2 (1-year EFS, 75.3% vs 72.7%, respectively; 2- and 3-year OS, 79% vs 71% [p = 0.904] and 84% vs 71%, respectively) [23, 30]. In APN311-303, 3-year EFS and OS were 24.1% and 54.7%, respectively, in patients with relapsed disease and 29.1% and 69.8%, respectively, in those with refractory disease [26]. For the group available for efficacy analysis in APN311-304, PFS and OS at 3 years was 31% and 66%, respectively [25]. In the Mueller et al. [22] study, PFS at 4.9 years was 33.1% and OS at 5.2 years was 47.7%. Median OS in the Wieczorek et al. [37] study was 33.1 months, and PFS and OS at 3 years were 75% and 86%, respectively.
Some studies separately evaluated survival outcomes for patients with relapsed and refractory disease receiving dinutuximab beta. In APN311-202 (stage I), survival outcomes were better for patients in the refractory group than for those in the relapsed group at 3 years (EFS, 44.6% vs 36.8%; OS, 62.5% vs 42.1%, respectively) [26]. Similarly, in APN311-303, EFS at 3 years in patients with refractory and relapsed disease was 29.1% versus 24.1%, respectively, and OS at 3 years was 69.8% versus 54.7%, respectively. There was a clear difference in survival benefit in the refractory group compared with the relapsed group in APN311-304, with 3-year PFS of 47% versus 19%, respectively, and with significantly better 3-year OS of 93% versus 50% (p = 0.015), respectively [25]. Mueller et al. [22] did not separately report data for the refractory group; however, survival was worse in patients with relapsed disease than in the whole cohort, which included patients with refractory disease (PFS and OS at 4.9 years: relapsed group, 18.1% and 41.2%; whole cohort, 33.1% and 47.7%, respectively). There was no statistically significant difference in the Wieczorek et al. [37] study in 1-year PFS between patients with refractory disease and those with relapsed disease (p = 0.27), most probably because of the low number of patients; however, more patients with refractory disease were progression free than those with relapsed disease.
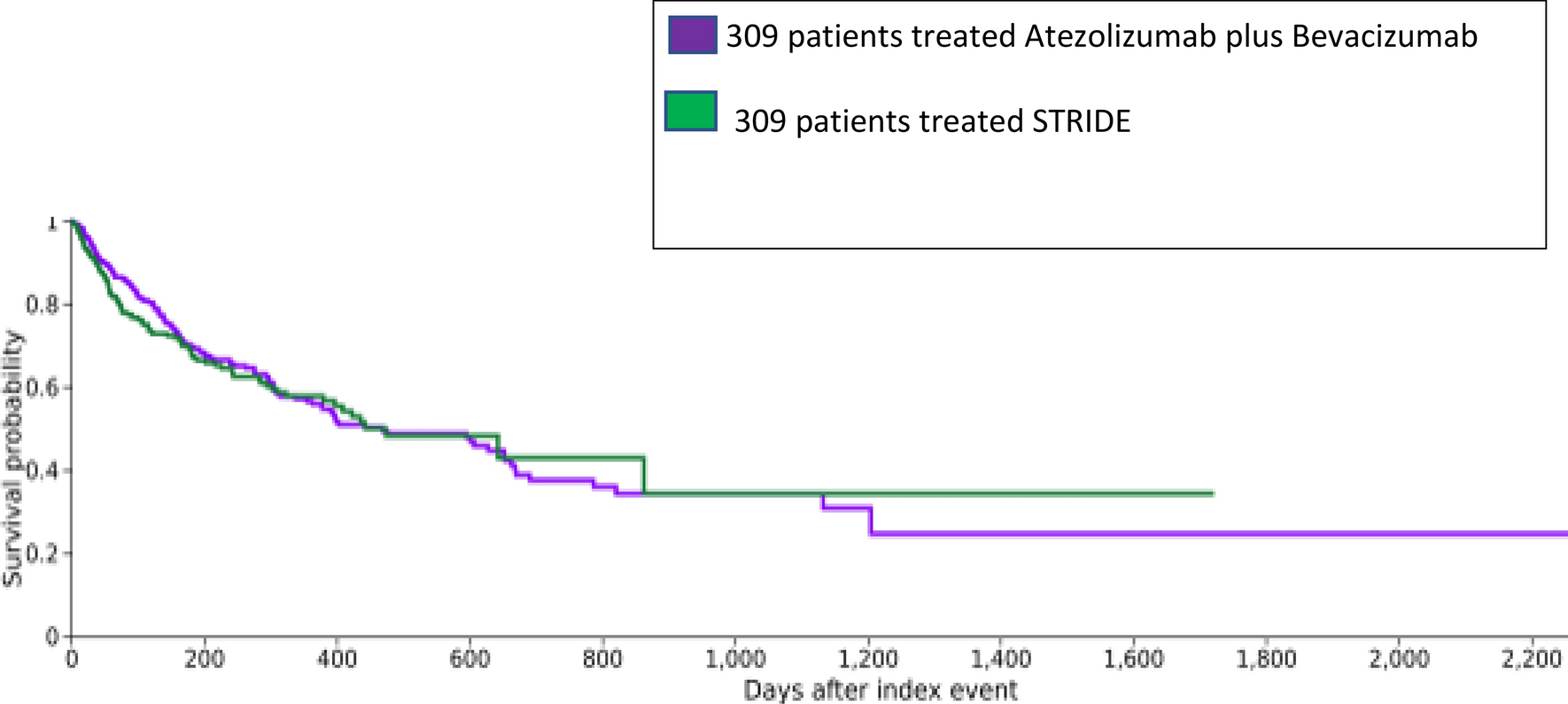
Findings from patients with relapsed disease only in APN311-303 [26] were compared with data from a historical cohort of patients with relapsed HR-NB who did not receive anti-GD2 immunotherapy from a registry study by Garaventa et al. [24]. OS at 3 years was 55% in the dinutuximab beta group and 24% in the historical control group (p = 0.0009) [26]. In a Cox model adjusted for prognostic factors for OS (i.e., age at diagnosis, gender, MYCN amplification, and INSS stage), OS remained statistically significantly higher in the group treated with dinutuximab beta (p = 0.002) [26].
In addition, comparative analyses for patients with relapsed disease were reported using pooled data from APN311-303 and APN311-202 (N = 48) versus two separate historical controls [26]. In a comparison versus the Garaventa et al. [24] registry data, 3-year OS was 50% versus 24% (p=0.0031), with an adjusted Cox model HR of 0.52 in favour of dinutuximab beta [
Comments (0)