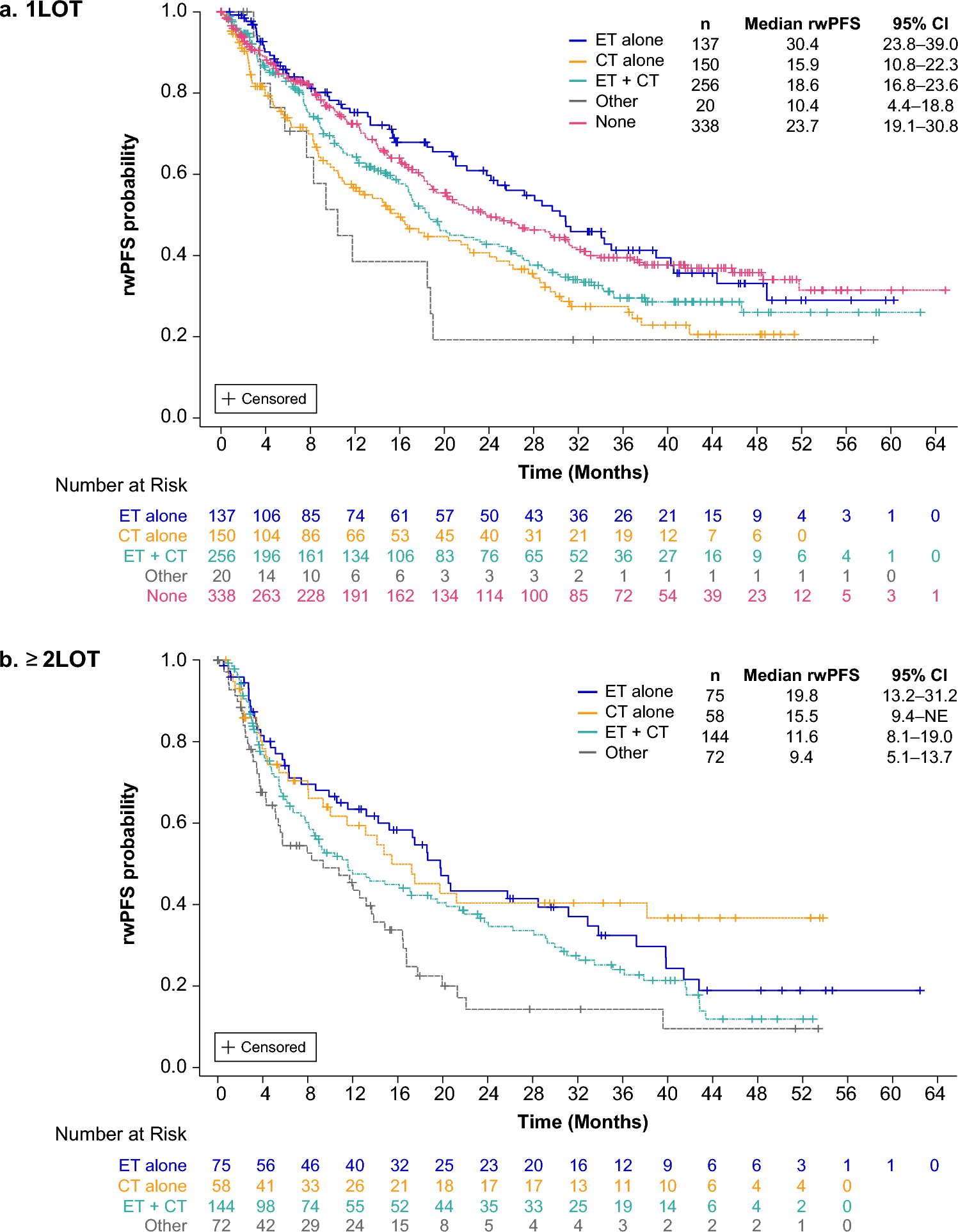
In this analysis of the POLARIS study, which by design allowed for comprehensive, prospective, and longitudinal patient data collection in routine clinical practice, we found that median rwPFS was numerically the longest in patients with HR+/HER2− ABC treated with palbociclib + ET who had received prior endocrine monotherapy, regardless of palbociclib LOT. Median OS also appeared to be longer (not reached) in patients with prior endocrine monotherapy in the 1LOT group after a median follow-up of approximately 39 months, but with no apparent OS difference in the ≥ 2LOT group. However, prior chemotherapy treatment either alone or with ET tended to be associated with less clinical benefit after initiating palbociclib. It is important to note that, as seen in PALOMA-3 and in other real-world studies [14, 19,20,21], palbociclib was still associated with a survival benefit across patients who had received different prior anticancer treatments, even in those who were heavily pretreated.
That patients who had received prior endocrine monotherapy tended to have better outcomes than those who had received other types of prior treatments may be suggestive of more endocrine-sensitive disease in these patients than in other prior treatment subgroups. These findings are consistent with a post hoc analysis of the PALOMA-3 trial [22], in which sensitivity to prior ET was also identified as a significant prognostic factor of prolonged OS with palbociclib treatment. In a real-world study by Franks et al. [15], which used electronic records of the Flatiron Health database to evaluate data from 5391 women diagnosed with HR+/HER2− ABC (2011–2020) [15], patients treated with prior chemotherapy (with or without ET and targeted therapies) or ET (with or without targeted therapies; no chemotherapy) had a greater risk of death than those with no prior anticancer treatment, with the prior chemotherapy group showing a greater risk (hazard ratio for death: 1.72; 95% CI 1.54–1.93) than the ET group (hazard ratio for death: 1.29; 95% CI 1.16–1.44). These findings align with those of our study in that prior ET alone may be associated with better outcomes for patients treated with first-line palbociclib than chemotherapy with or without ET. However, in our study, median rwPFS was longer, and the median OS was generally comparable between those with prior ET alone and those with no prior treatments. These inconsistent findings could be related to the substantial differences in characteristics of the study populations, including the sample size, younger age, and higher visceral disease prevalence, in the population of Franks et al. [15], as well as prevalence of recurrent versus de novo disease (not reported in the other study) in addition to other variations between study populations and subgroups.
While the differences in clinical outcomes observed across the different types of prior anticancer treatments may be due to prior treatment-related effects on palbociclib effectiveness, they could also be related to patient and disease characteristics associated with prior treatment choices. For instance, patients treated with prior endocrine monotherapy tended to be older than those treated with prior chemotherapy in both the 1LOT and ≥ 2LOT groups. This may reflect physicians’ desire to avoid chemotherapy in older patients due to greater prevalence of comorbidities, frailty, and increased risk of chemotherapy toxicity; geriatric assessments are recommended to guide treatment selection in older patients with cancer [23]. Furthermore, multiple studies have shown that patients diagnosed with breast cancer at a younger age can have more aggressive disease and poor survival compared with those diagnosed at an older age [24,25,26,27], but that they may respond better to chemotherapy than older patients [24, 27]. In the PALOMA-3 post hoc analysis [22], investigators also found that patients who received chemotherapy in the ABC setting prior to receiving palbociclib were younger than those without prior chemotherapy and had shorter median durations of PFS and OS. Multiple other real-world studies of patients with HR+/HER2− ABC have additionally reported that chemotherapy treatment prior to palbociclib in any setting was associated with worse survival outcomes [14, 15, 28, 29].
Except for the prior-chemotherapy-alone subgroup, shorter median TFI correlated with a shorter median rwPFS in this POLARIS analysis. This is consistent with the findings of several other studies, including a systematic literature review, of patients with HR+/HER2− ABC that have reported a shorter TFI or disease-free interval as prognostic of worse post-recurrence survival [13, 30]. Contrastingly, in the prior-chemotherapy-alone subgroup, a longer median TFI (> 12 months) was associated with a shorter median rwPFS, while those with a shorter TFI (≤ 12 months) had a longer median rwPFS (14.5 months versus 22.1 months). This disparate observation in the prior-chemotherapy-alone subgroup may be due to several factors, most notably, as aforementioned, that this subgroup included a larger percentage of younger patients (1LOT: 25% < 50 years of age) compared with the other prior-treatment groups (< 50 years range: 5–15%). Another hypothesis for the shorter clinical benefit of palbociclib seen in patients treated with prior chemotherapy may be that their cancer had become less hormone responsive or more ET resistant. A small study of patients with estrogen receptor-positive metastatic breast cancer has reported that treatment with adjuvant chemotherapy led to acquired mutations, as well as chemotherapy-induced selection of preexisting mutations, in genes that increase the risk of ET resistance [31]. Further research assessing patient characteristics and how they influence prior anticancer treatment decision in the real-world setting is warranted to better differentiate the relationship of prior chemotherapy treatment on possible mechanisms of resistance to future palbociclib + ET treatment.
Per-label use of palbociclib aligns with guidelines for the treatment of HR+/HER2− ABC; a CDK4/6 inhibitor + AI is recommended as 1LOT for patients with treatment-naïve HR+/HER2− ABC, while a CDK4/6 inhibitor in combination with fulvestrant is recommended for patients whose disease progressed following prior ET [5,6,7]. When we looked at clinical outcomes by prior treatments in the population treated per label, the findings were generally directionally consistent with those in the overall POLARIS population, except that patients who had received prior chemotherapy alone prior to palbociclib 1LOT had longer rwPFS and OS than seen in the overall population. A potential explanation for the better outcomes seen in the per-label population 1LOT group treated with chemotherapy alone may be related to the large percentage of patients treated with palbociclib + fulvestrant who were excluded (42%; 129/308) from the 1LOT group because they had not received prior ET (as per the palbociclib label) [7, 10]. As a result, patients included in the chemotherapy-alone subgroup in the per-label population were essentially treated with palbociclib + AI, among which de novo disease was more prevalent [10]. Patients with de novo HR+/HER2− ABC treated with a CDK4/6 inhibitor and ET have been found in several clinical trials and real-world studies to have better survival outcomes than those with recurrent disease [32]. In the overall POLARIS population treated with 1LOT palbociclib, most (93%; 533/573) patients in the 1LOT group received palbociclib + AI as per-label and according to treatment guidelines; however, only 58% (179/308) of patients received palbociclib + fulvestrant after prior ET use [6, 7, 10]. Exact reasons for such a large proportion of patients in the overall POLARIS population treated with 1LOT palbociclib + fulvestrant in the absence of prior ET use as per label is unknown, but possible reasons could include tolerability issues or the preferences of physicians/patients alongside other patient and disease characteristics. In the ≥ 2LOT group, less than half (43%; 149/349) of patients were treated per label, mostly because they received palbociclib + AI [6, 7, 10]. Furthermore, 17% (58/349) had only received prior chemotherapy and had no prior ET. Further study is warranted on the real-world treatment patterns of CDK4/6 inhibitors and adherence to treatment guidelines.
Generally, treatment guideline recommendations for early HR+/HER2− breast cancer include surgery with or without neoadjuvant chemotherapy, radiation therapy, and adjuvant ET with or without chemotherapy, which is typically reserved for patients at higher risk of recurrence [4, 33, 34]. Data from this POLARIS analysis suggest that chemotherapy alone or combined with ET are the predominant prior treatments received in patients with HR+/HER2− breast cancer (> 70% in 1LOT palbociclib group with prior treatment [> 90% with recurrent disease] and > 57% in ≥ 2LOT palbociclib), especially among younger patients. These study findings differ from those of other studies that have evaluated treatment patterns prior to palbociclib treatment, which have reported higher proportions of patients treated with prior ET alone and lower proportions treated with chemotherapy alone [14, 15]. However, comparisons across studies are difficult since population characteristics widely varied, as did study years. As stated in guidelines, treatment decisions for patients diagnosed with HR+/HER2− breast cancer should be individualized with consideration of genetic factors, response to surgery and other past treatments, patient characteristics, comorbidities, patient preferences, etc. [4, 33, 34]. As the treatment journey of patients with HR+/HER2− breast cancer becomes longer and more complex with extended survival durations in the evolving therapeutic landscape [35,36,37,38], treatment sequencing may require optimization to not adversely impact the effectiveness of therapies received later in the course of disease. Further research is warranted to improve our understanding of patient and disease characteristics associated with treatment decisions in routine clinical practice.
4.1 Limitations
In this real-world observational study with no control group, effectiveness but not causality could be established between treatment and outcomes. Patient treatments and sequencing were determined by the treating physician, which may have led to potential selection bias. Furthermore, disease progression may have not been assessed on a schedule as in clinical trials and on the basis of Response Evaluation Criteria in Solid Tumors; therefore, these data are limited by the individual treating clinician’s interpretation of radiographic scans or pathology results. In this study, no balancing of patient and disease characteristics between the prior treatment subgroups was performed, limiting the interpretation of any associations between prior anticancer treatments and clinical outcomes. Additionally, characterization of breast cancer subtype beyond HR and HER2 status (e.g., luminal, basal, or HER2 enriched) or HR expression level were not collected in this real-world observational study. Also, some prior-treatment subgroups had relatively few patients. Because this study was based on health records from real-world clinical practice, there was the possibility for missing or inaccurate data. Lastly, the results of this study may not be generalizable to patients with HR+/HER2− ABC outside the USA and Canada.

Comments (0)