
Remember me
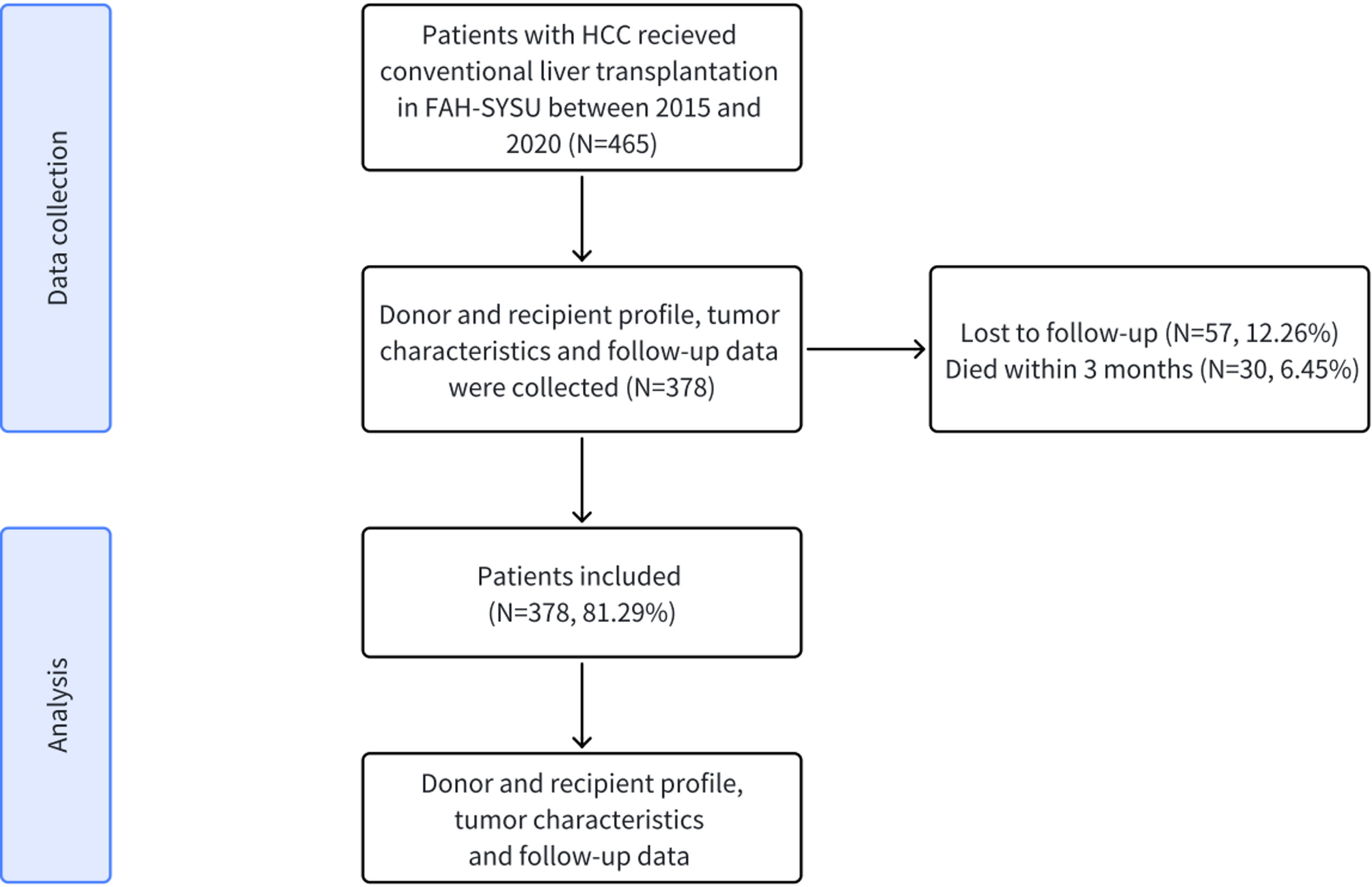



A total of 378 patients with HCC who underwent LT were included in the study. The baseline clinical and demographic characteristics of 378 recipients and donors comprising the cohort are summarized in Table 1. The mean age of recipients was 51.4 years, 346 (91.5%) were men, and the mean BMI was 23.4. Hepatitis B (314, 83.1%) and Hepatitis C (36, 9.5%) was the most common etiologies in recipients, followed by other (24, 6.4%). Pre-transplantation, patients diagnosed with HBV or HCV infection receive continuous antiviral therapy and undergo regular testing for HBV-DNA and HCV-RNA to ensure the absence of viral replication prior to surgery. Patients will continue to receive the same antiviral therapy post-transplantation as they did pre-transplantation. Post-transplantation patients are routinely monitored through regular testing for eight serological tests including hepatitis B surface antigen (HBsAg), hepatitis B surface antibody (anti-HBs), hepatitis C antibody (anti-HCV), human immunodeficiency virus antibody (anti-HIV), syphilis antibody (TP-Ab), HBV-DNA and HCV-RNA to confirm the absence of viral activity. Serologic assessments following transplantation revealed no indications of viral activity. The median preoperative ALT and AST was 23 U/L (IQR 35–53) and 46 U/L (IQR, 34-74.5), respectively. The number of Child-Pugh grade of A (39.7%) recipients was 150, and 203 (53.7%) had a grade of B, while 25 (6.6%) patients had a grade of C. Most of donors were DBD (314, 83.1%). Additionally, the mean cold ischemia time was 6.8 h. For surgery details, the mean anhepatic phase was 56.4 min, the mean total surgery time was 462 min and the median intraoperative blood loss was 1500 ml (Table 1).
Table 1 Donor characteristics, recipient characteristics, tumor characteristics, surgical details, and patient outcomes after transplantationTumor characteristics and patient outcomesIn this cohort, 225 (59.5%) patients were beyond Milan criteria at diagnosis, and 197 (52.1%) were beyond UCSF criteria. The AFP values, tumor size and number of HCC are shown in Table 1. A total of 102 (27%) patients had AFP levels greater than 400 ng/ml, 134 (35.4%) patients had more than 3 tumors, and 147 (38.9%) patients had tumor sizes greater than 50 mm. Some patients underwent TACE (152, 40.2%), ablation (101, 26.7%), and liver resection (62, 16.4%) before transplantation. On explant pathology, 112 (29.6%) patients had tumor microvascular invasion (MVI). HCC recurrence was observed in 165 (43.7%) patients. Median RFS was 92.18 months (IQR, 11.8–66.2), with recurrence-free rates of 75.9% at 1 year, 60.8% at 3 years, 56.1% at 5 years (Fig. 2B). 239 (63.2%) patients remained alive following transplantation, and the median overall survival was 100.75 months, with survival rates of 90.5% at 1 year, 71.2% at 3 years, 66.3% at 5 years (Fig. 2A).
Fig. 2
Overall survival and recurrence-free survival of HCC patients after liver transplantation. (A) Overall survival. (B) Recurrence-free survival
Univariate analysis of overall survival and recurrence-free survivalUnivariate cox regression analysis showed that pretransplant AST > 100 U/L (HR: 1.933, 95%CI, 1.312–2.849, P = 0.001), AFP > 400 ug/L (HR: 2.649, 95%CI, 1.891–3.711, P < 0.001), and maximum tumor diameter > 30 mm (HR: 2.095, 95%CI, 1.398–3.139, P < 0.001) were risk factors affecting the overall survival of patients, and the overall survival of patients after transplantation would also be affected when the tumor stage was beyond the UCSF standard (HR: 1.417, 95%CI, 1.011–1.988, P = 0.043) and the tumor MVI (HR: 3.130, 95%CI, 2.241–4.371, P < 0.001). At the same time, the postoperative complications of EAD (HR: 2.805, 95%CI, 2.008–3.919, P < 0.001), AR (HR: 5.517, 95%CI, 3.901–7.803, P < 0.001), and BC (HR: 2.569, 95%CI, 1.831–3.604, P < 0.001) were associated with the overall survival of patients. Tumor downstaging by preoperative neoadjuvant therapy is a protective factor for long-term survival of patients (Table 2).
Table 2 Univariate analyses of risk factors for overall survival and Recurrence-free survival in the entire cohortCox regression analysis was performed to examine RFS in the entire cohort. Univariate cox regression analysis showed that AST > 100 umol/L (HR: 2.362, 95%CI, 1.665–3.351, P < 0.001), AFP > 400 ug/L (HR: 2.676, 95%CI, 1.960–3.655, P < 0.001), maximum tumor size > 30 mm (HR: 2.823, 95%CI, 1.890–4.217, P < 0.001), tumor stage beyond UCSF criteria (HR: 1.603, 95%CI, 1.172–2.193, P = 0.003) and MVI (HR: 3.435, 95%CI, 2.524–4.675, P < 0.001) were also risk factors for recurrence-free survival. Similarly, tumor staging beyond Milan criteria (HR: 1.631, 95%CI, 1.174–2.267, P = 0.004), donor liver cold storage time > 10 h (HR: 1.576, 95%CI, 1.054–2.357, P = 0.027), and AR (HR:5.375, 95%CI, 3.563–8.110, P < 0.001) after transplantation will lead to an increased risk of tumor recurrence (Table 2). The survival analysis of patients with EAD, AR and BC after liver transplantation showed that the overall survival and recurrence-free survival of patients with liver cancer were significantly affected by EAD (P < 0.0001), AR (P < 0.0001) and BC (P < 0.001) (Fig. 3A and F).
Fig. 3
Effects of EAD, AR and BC on overall survival and recurrence-free survival after liver transplantation. (A) Impact of EAD on overall survival (B) Impact of AR on overall survival (C) Impact of BC on overall survival (D) Impact of EAD on recurrence-free survival (E) Impact of AR on recurrence-free survival (F) Impact of BC on recurrence-free survival
Multivariable predictors of HCC patient overall survival and recurrence-free survival outcomesMultivariable regression analysis was performed to identify independent risk factors for overall survival and recurrence-free survival after LT. Among the evaluated factors, AR (HR: 3.439, 95%CI, 2.244–5.270, P < 0.001) had the largest hazard ratio for the risk of overall survival among all risk factors. AFP > 400 ug/L (HR: 1.667, 95%CI, 1.152–2.416, P = 0.007), MVI (HR: 1.749, 95%CI, 1.218–2.511, P = 0.002), and EAD after transplantation (HR: 1.635, 95%CI, 1.143–2.340, P = 0.013) were independent risk factors associated with patient overall survival (Table 3). Results of other univariate analyses, including AST > 100 umol/L, UCSF criteria, tumor size, were not significantly associated with overall survival. However, in the multivariate analysis of recurrence-free survival of tumor patients, AR after transplantation (HR: 5.141, 95%CI, 3.425–7.718, P < 0.001), AFP > 400 ug/L (HR: 1.642, 95%CI, 1.117–2.299, P = 0.004), MVI (HR: 1.890, 95%CI, 1.357–2.632, P < 0.001) and maximum tumor diameter > 30 mm (HR: 1.564, 95%CI, 1.010–2.422, P = 0.045) were the independent risk factors for RFS (Table 3).
Table 3 Multivariate analyses of risk factors for overall survival and recurrence-free survival in the entire cohort
Comments (0)