
Remember me



In this large cohort study, we found that relying solely on the preoperative cN stage was insufficient for accurately predicting the postoperative pN stage. In particular, the preoperative cN1 stage demonstrated low sensitivity and PPV, which poses challenges in reliably identifying the pN1 status. In the treatment of HCC, the inability to accurately predict pN1 suggests that the current staging system may not be entirely precise. Therefore, careful consideration of this factor in clinical decision-making is essential.
The discrepancy between cN1 and pN1 has also been reported in previous studies. According to a report by Mo et al., when abdominal CT was used to distinguish LNM based on a 10 mm cutoff, the sensitivity was higher at 75.9%, but the specificity was lower at 53.5% [16]. However, this study involved a small sample size, and the criterion for determining cN1 was limited to a 10 mm tumor size. In contrast, our study, which was a large-scale cohort analysis, allowed for a more in-depth examination of the mismatch between cN1 and pN1. Another cohort study using the NCDB included 1,442 HCC patients who underwent hepatectomy with LND. Patients who underwent LND had higher clinical T and N stages, with cN1 status predicting pN1 status. Despite the high NPV of 97.9% for cN1, its PPV remained relatively low at 56.3%. However, owing to its high NPV, the study suggested considering LND only for patients with cN1 status [4]. However, it is important to also consider the potential for missed pN1 cases in clinical surveillance.
Our study identified several risk factors for cN1 and pN1. The factors associated with cN1 included age, female sex, white ethnicity, fibrolamellar type, spindle cell variant, clear cell type, HCC-CCA, tumor size, cT stage, region, and grade. The factors associated with pN1 included age, female sex, fibrolamellar type, spindle cell variant, pleomorphic type, HCC-CCA, cT stage, region, and grade. Common factors between cN1 and pN1 included age, female sex, fibrolamellar type, spindle cell variant, HCC-CCA, cT stage, region, and grade. Notably, the utilization of a nationwide multicenter cohort enabled us to explore the associations between LNM and rare histological subtypes, such as the fibrolamellar type and HCC-CCA. These findings underscore the complexity of predicting pN1 status in HCC patients and emphasize the need for comprehensive risk assessment beyond the preoperative cN stage. Further research into the clinical risk factors associated with cN1 and pN1 is crucial to improve patient stratification and guide optimal treatment strategies.
Previous studies have extensively investigated risk factors associated with LNM in HCC. For example, a study utilizing the Surveillance, Epidemiology, and End Results (SEER) database examined prognostic factors in HCC patients with LNM. Variables such as grade, T stage, liver surgery, chemotherapy, radiation therapy (RTx), AFP level, fibrosis score, tumor size, and M stage were assessed. This study revealed that appropriate clinical management strategies could be developed for HCC patients with LNM [17]. Another study involving 2,034 HCC patients reported that preoperative carcinoembryonic antigen levels exceeding 10 ng/mL were associated with a higher incidence of LNM. Larger tumor size, vascular invasion, higher histologic grade, and lack of encapsulation are also correlated with LNM [8]. Clinical data from 268 HCC patients were used to develop a nomogram for predicting LNM. Furthermore, studies using serologic biomarkers, including the neutrophil-to-lymphocyte ratio (N/L ratio), platelet count, prothrombin time, and total protein, have demonstrated good performance in predicting LNM [13, 14].
Additionally, experimental research in HCC has identified several biomarkers for LNM, such as the nuclear accumulation of CXCR4, the overexpression of VEGF-C and CK19, and hypoxia-inducible factor 1-alpha (HIF-1α). These biomarkers, along with gene expression profiling, have provided new insights into the molecular mechanisms underlying LNM. Moreover, miRNA-based models have been shown to be reliable for the early prediction of LNM in HCC patients [18,19,20,21].
Despite its common occurrence, the clinical significance of LNM in HCC treatment is often underestimated. LNM significantly impacts survival outcomes, as demonstrated by an autopsy study involving 660 HCC patients, which revealed a substantial LNM incidence of 25.5%. Larger tumors (> 10 cm) were associated with a 40% LNM incidence, and poorly differentiated tumors with sinusoidal growth patterns presented higher LNM rates [6]. In addition, a study examining 342 HCC patients with extrahepatic metastases revealed that LNM was the second most prevalent type of metastasis following lung metastasis [22, 23].
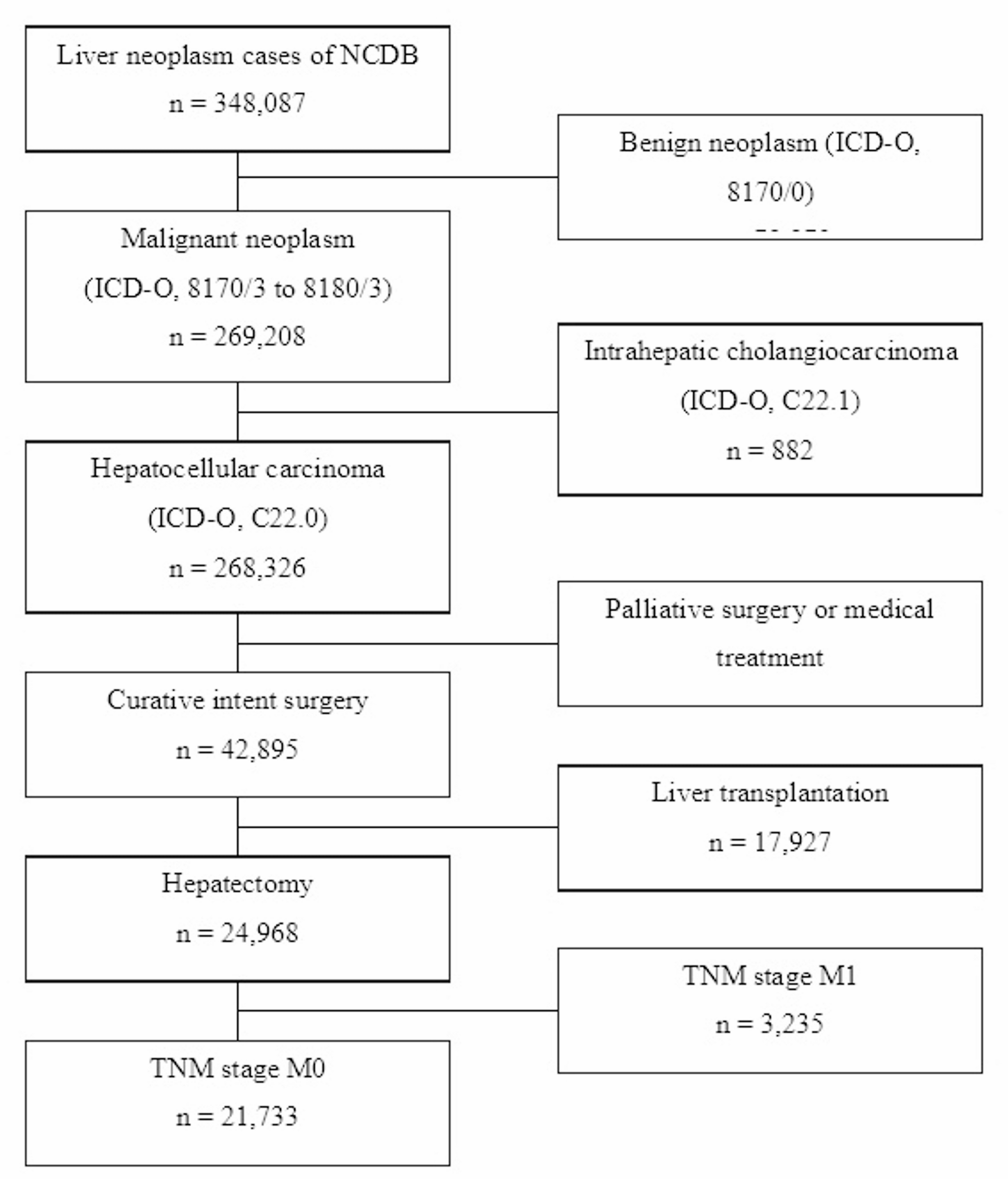
In this study, we excluded patients with distant metastasis which exerts a dominant influence on survival outcomes, regardless of LNM. Including M1 cases could introduce significant confounding bias when assessing the independent prognostic impact of LNM. Similarly, patients who underwent liver transplantation were excluded due to their distinct clinical characteristics compared to those undergoing hepatic resection. Liver transplantation is typically reserved for patients with more advanced hepatic dysfunction and different baseline prognostic factors, and it is associated with higher morbidity and mortality than hepatic resection. Including these cases could therefore increase selection bias and confound the interpretation of survival outcomes. However, the exclusion of M1 and liver transplantation cases may limit the generalizability of our findings to the broader HCC population.
Selective LNE in HCC patients has been subjected to scrutiny, with postoperative confirmation of LNM in 18 out of 2189 patients (0.8%). Importantly, no mortalities or occurrences of liver failure were reported. Patients with solitary LNMs presented a more favorable prognosis than did those with multiple LNMs, with a median survival of 29 months and one-, three-, and five-year overall survival rates of 85%, 42%, and 21%, respectively [24]. A nationwide survey conducted in Japan investigated 14,872 HCC patients who underwent surgical resection, employing the Japanese staging system. Notably, LNM was associated with a better one-stage prognosis than distant metastasis [3]. This systematic review included 603 HCC patients and 434 intrahepatic cholangiocarcinoma (ICC) patients, revealing a 51.6% prevalence of LND and a 15.2% incidence of LNM in HCC patients and a 78.5% LND rate with a 45.2% incidence of LNM in ICC patients. Routine LND is advocated for both HCC and ICC [25]. In patients with HCC with LNM, aggressive locoregional treatment alongside LND has yielded relatively favorable outcomes. Regional lymphadenectomy is considerably safe and has a low intraoperative complication rate [12, 26]. Among the 15 patients, four experienced lymph node recurrence, and 13 experienced intrahepatic recurrence. The median survival after LND was 25.2 months [27]. These findings highlight the importance of proactive therapeutic strategies in managing HCC patients with LNM and underscore the potential benefits of interventions such as transcatheter arterial chemoembolization (TACE), RTx, and selective LND in improving patient outcomes. However, it is important to recognize that HCC with LNM is indicative of more advanced disease. According to the Barcelona Clinic Liver Cancer staging system, patients with LNM are classified as having advanced HCC, which typically requires systemic treatment. Systemic therapies, including tyrosine kinase inhibitors and immune checkpoint inhibitors, play crucial roles in the management of advanced-stage HCC, aiming to improve survival and control disease progression. Thus, the presence of LNM should prompt consideration of not only locoregional interventions but also systemic treatment strategies in the comprehensive management of advanced HCC [28].
Conversely, a body of literature suggests that LND may not be warranted in cases of HCC. An analysis leveraging SEER data concluded that while LNM serves as a prognostic factor in HCC, routine LND is deemed superfluous. Among 8,829 HCC patients, 1,346 underwent LND, with LNM detected in 56 individuals (4.2%). Among the 2,497 lymph nodes examined, 93 (3.7%) tested positive for LNM. Factors such as race, tumor size, clinical T stage, extrahepatic bile duct invasion, and tumor grade were identified as risk factors for LNM [2]. Another study focusing on LND for HCC patients with LNM performed LND in 968 operable patients reported lymph node enlargement. LNM was confirmed in 41 individuals (5.1%). Among the 49 patients with confirmed LNM, those who underwent complete LND had one-, three-, and five-year survival rates of 68.0%, 31.0%, and 31.0%, respectively. However, there was no significant difference in survival curves between those who did and did not undergo LND (p = 0.944) [26]. These discrepancies may arise from differences in patient selection, extent of LND, follow-up duration, and analytical methods. Notably, prior studies focused exclusively on patients undergoing LND, which may introduce selection bias. In contrast, our study analyzed a broader patient population, reflecting real-world practice.
Certain histological classifications, such as the fibrolamellar type or HCC-CCA, are associated with LNM, and LND is often more actively recommended [5, 29,30,31]. In a comparison of combined HCC-CCA, HCC, and ICC, a greater frequency of LNM was observed in combined tumors, which presented a poorer prognosis than did HCC. However, ICC has the worst prognosis, positioning combined tumors as having an intermediate clinical profile between those of ICC and HCC [31]. Furthermore, when posttreatment outcomes of ICC and HCC patients were assessed, academic cancer centers demonstrated superior survival rates compared with community cancer centers [32]. This study suggested that previously unknown spindle cell variants and pleomorphic types may be related to LNM.
Overall, recent studies emphasize the importance of considering LNM in HCC treatment strategies and underscore the potential benefits of interventions such as TACE, RTx, and selective LND. Future research should continue to investigate the clinical and molecular factors associated with LNM in HCC patients to optimize treatment approaches and improve patient outcomes.
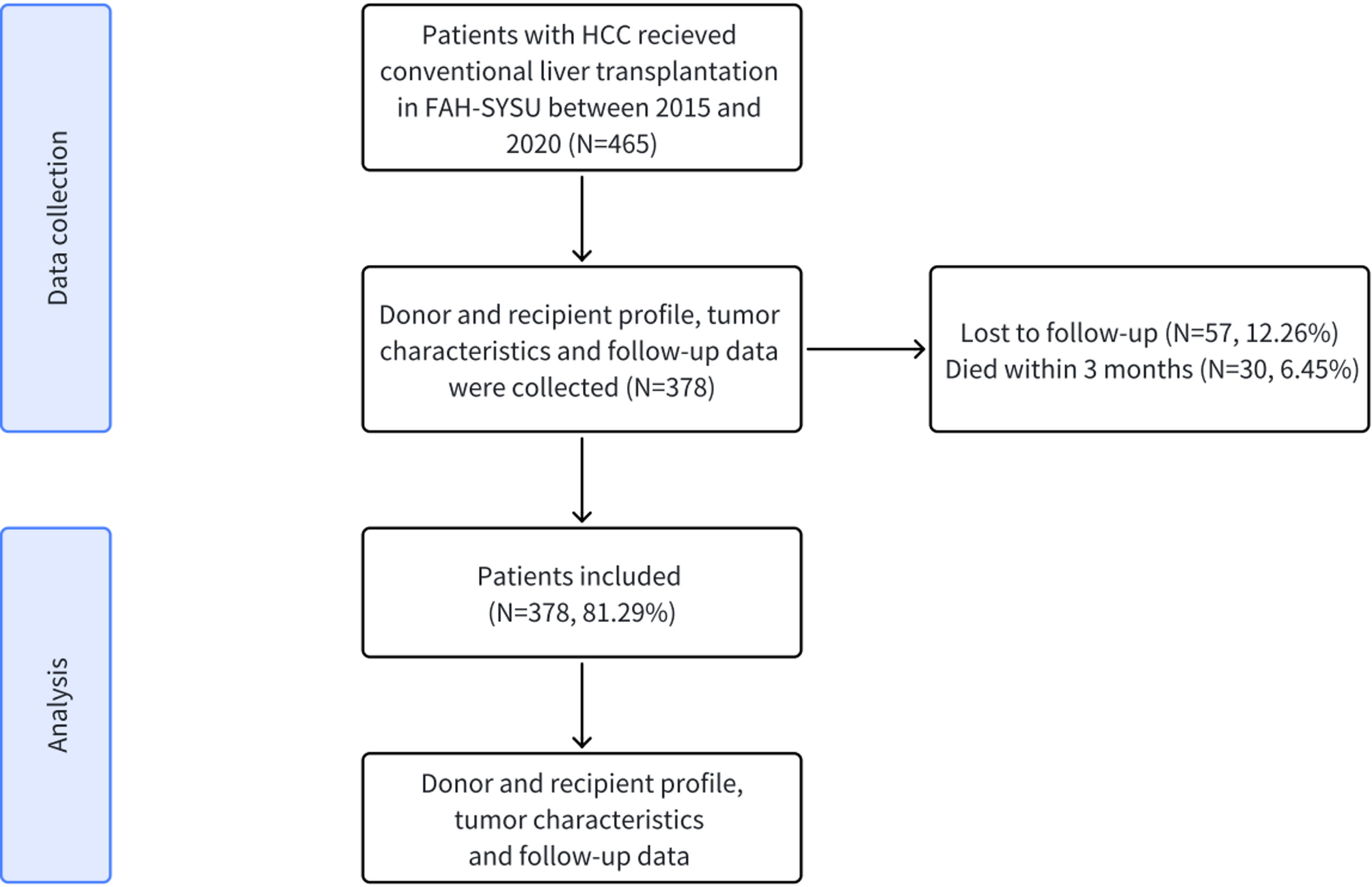
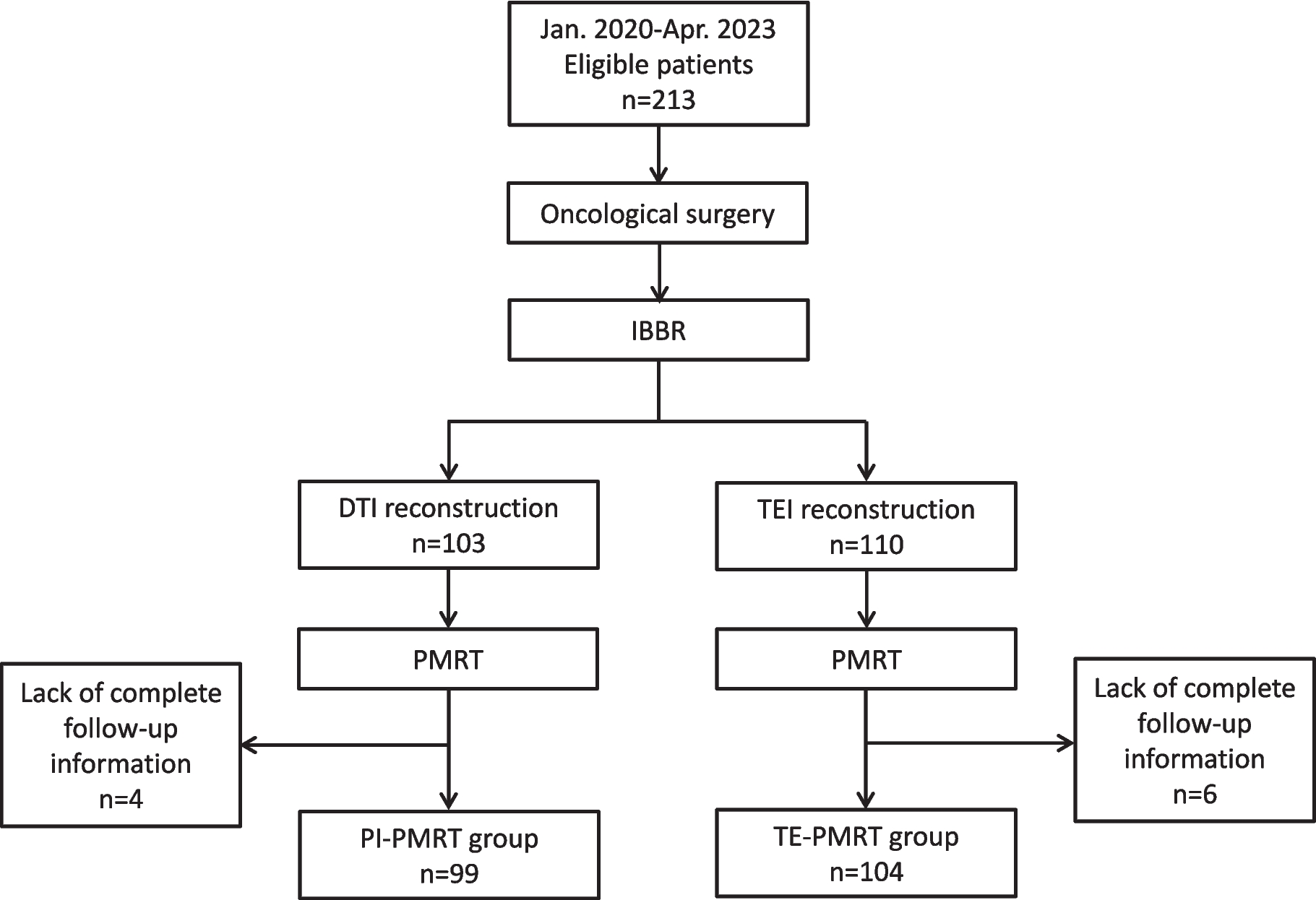
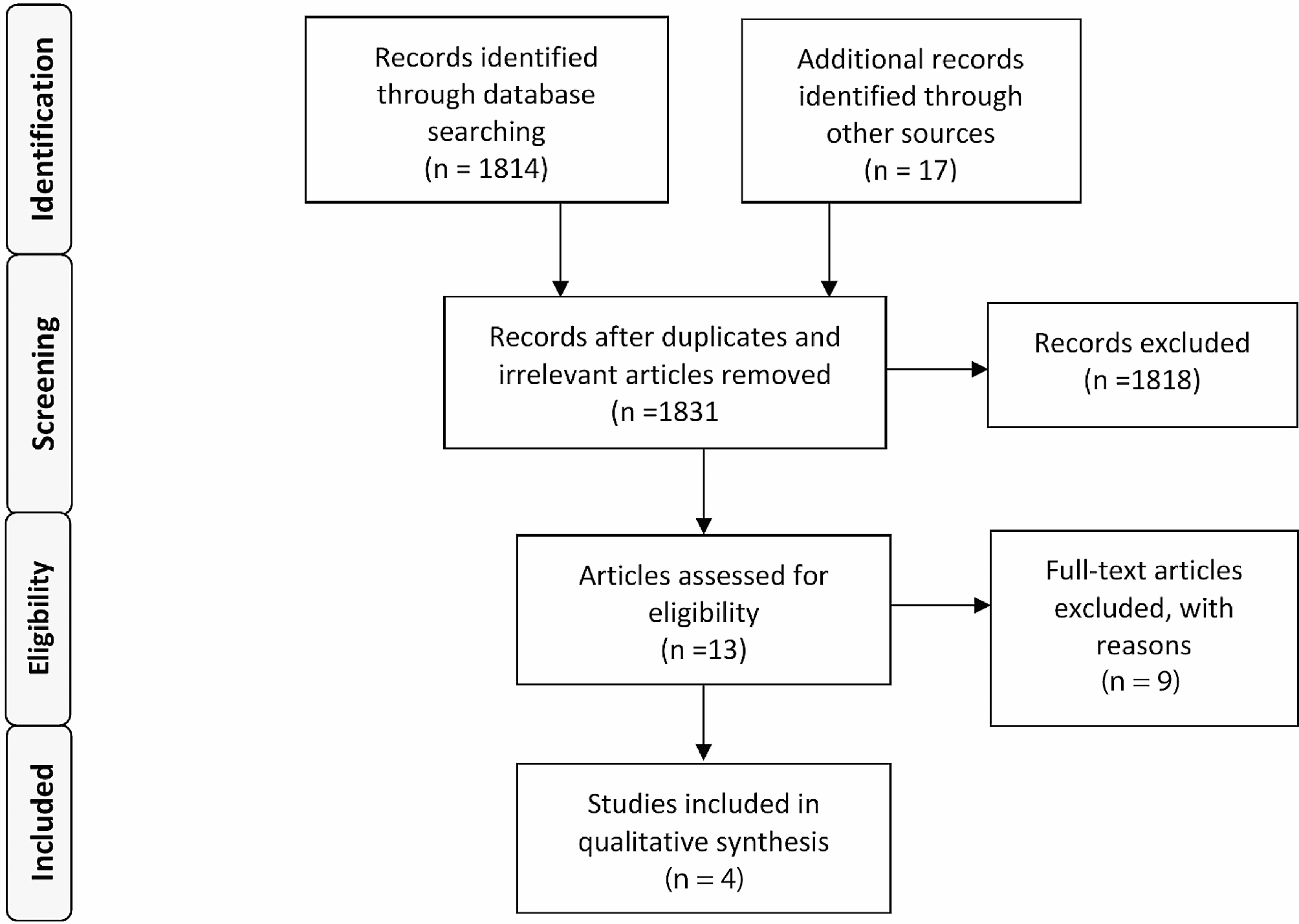
Fig. 1
Flow-chart of patient selection
Comments (0)