
Remember me



This study was a single-center retrospective cohort analysis involving bladder cancer (BC) patients who underwent either ELRC or TLRC procedures. Data were collected from the Department of Urology, the Affiliated Hospital of Qingdao University, from January 2020 to January 2025. The study protocol was approved by the Ethics Committee of the Affiliated Hospital of Qingdao University (approval number: QYFYEC2023-67) and was registered with the “Chinese Clinical Trial Registration and Information System” (registration number: MR-37-23-039856). All participants provided informed consent in compliance with the Declaration of Helsinki.
Patient populationTotal 298 BC patients, aged between 18 and 85 years, were enrolled in this study. Among these patients, 202 (67.79%) underwent ELRC, while 96 (32.21%) underwent TLRC. Patients were stratified according to the 2023 updated European Association of Urology (EAU) guidelines. A definitive pathological diagnosis was obtained for all patients before opting for radical cystectomy. Preoperative evaluations included enhanced computed tomography (CT) urography, chest CT, and abdominal ultrasonography to detect nodules or distant metastases. Magnetic resonance imaging (MRI) or 18 F-FDG PET/CT was employed when CT results were inconclusive. The decision to perform ELRC or TLRC was made based on a combination of surgeon preference, patient anatomy, and clinical characteristics. Patients with no history of major intra-abdominal surgery, lower BMI (< 40 kg/m²), and organ-confined disease without bulky pelvic lymphadenopathy were considered suitable candidates for ELRC. TLRC was preferred in cases where complex pelvic anatomy was present. Additionally, during the early study period, TLRC was more commonly used due to the limited availability of standardized extraperitoneal instrumentation and training.
Inclusion criteria were as follows: (1) Age between 18 and 85 years, irrespective of sex, with an expected life expectancy of at least 24 months; (2) Informed consent was waived due to the retrospective design, but patients were informed of data usage according to institutional policy; (3) American Society of Anesthesiologists (ASA) classification I–IV; (4) Clinical diagnosis of BC confirmed by imaging and pathology; (5) No significant abnormalities in vital organs such as liver, kidney, bone marrow, and heart, indicated by laboratory parameters including aspartate aminotransferase (AST) and alanine aminotransferase (ALT) ≤ 2.5 upper limit of normal (ULN), albumin ≥ 25 g/L, serum creatinine ≤ 1.5 ULN, white blood cells ≥ 3.5 × 10^9/L, neutrophils ≥ 1.5 × 10^9/L, hemoglobin ≥ 90 g/L, platelets ≥ 80 × 10^9/L, and electrocardiogram without significant clinical abnormalities.
Exclusion criteria included: (1) History of major abdominal surgery or chronic bowel disease; (2) Body mass index (BMI) > 40 kg/m²; (3) Severe cardiovascular disease; (4) Immunodeficiency or history of organ transplantation; (5) History of severe central nervous system (CNS) disorders; (6) Concurrent urological diseases that contraindicate radical cystectomy; (7) Pregnancy or lactation; (8) Uncontrolled epilepsy, CNS disorders, or psychiatric disorders; (9) History of cerebral infarction or hemorrhage within the past six months; (10) Severe recurrent uncontrolled infections or other severe uncontrolled comorbidities.
Exclusion criteria during the study period were as follows: (1) Significant missing primary data; (2) Poor compliance, defined as failure to adhere to planned follow-ups or missing more than two follow-ups; (3) Participants deemed unsuitable for continuing the study due to adverse events, as judged by the investigator; (4) Participants or their legal representatives voluntarily requesting withdrawal from the study or discontinuation of treatment at any stage; (5) Sudden preoperative onset of severe comorbidities, making the patient unsuitable or unable to undergo the planned surgical procedure; (6) Changes in patient conditions necessitating emergency rather than elective surgery, confirmed by the attending physician; (7) Receipt of treatment deviating from the study protocol.
Preoperative managementFor patients with ileal conduit and ileal orthotopic neobladder (ION), bowel preparation was needed. Oral antibiotic was used for 3 days before operation. Liquid diet was administered for 2 days before operation. Oral laxative was performed for 1 day prior to surgery. Stable blood pressure and blood glucose < 10mmol/L were required. Under ERAS, high energy drinks were recommended for 4 h before operation (exclude diabetes). Antibiotic prophylaxis was administered intravenously 30 min before surgery. Bowel preparation was performed only for patients undergoing ileal orthotopic neobladder or ileal conduit. Patients receiving cutaneous ureterostomy did not undergo bowel preparation, as the procedure does not involve bowel manipulation. All patients were managed using an ERAS protocol developed in accordance with international guidelines, including the ERAS Society recommendations for urologic surgery. Key components included early ambulation, early enteral nutrition, multimodal analgesia, and avoidance of nasogastric tubes and prolonged drainage.
Surgical techniqueBuilding on prior foundational work and incorporating insights from both domestic and international literature and guidelines, our team continuously refined and optimized the surgical approach. A standardized protocol for ELRC was established, allowing for systematic comparison. The key procedural steps were defined as follows: (1) Expansion of the extraperitoneal space; (2) Expansion of the iliac fossa; (3) Mobilization of the spermatic cord; (4) Transection of the spermatic cord; (5) Transection of the umbilical artery; (6) Dissection and transection of the ureter; (7) Dissecting the peritoneum along the vas deferens; (8) Dissecting the opposite side; (9) Converging posterior to the prostate; (10) Dissecting the peritoneum along the posterior aspect of the bladder; (11) Transection of the dorsal vein complex (DVC); (12) Transection of the urethra; (13) Pelvic lymphadenectomy; and (14) Urinary diversion. A 2–3 cm infraumbilical midline incision was made to create an extraperitoneal working space using blunt finger dissection and a balloon dilator. A total of five trocars were placed in a fan-shaped distribution: 10 mm camera port infraumbilically. Two 12 mm working ports at the bilateral lower quadrants (midclavicular line, ~ 2 cm below the umbilicus). Two 5 mm assistant ports lateral to the rectus margin. Meticulous dissection was carried out to preserve the integrity of the peritoneum, especially in step 3, 7 and 8. After bladder excision and lymphadenectomy, a transperitoneal approach was utilized to facilitate urinary diversion for an ileal neobladder or an ileal conduit by opening the peritoneum under direct visualization.
Intraoperatively, careful attention was given to preserving the integrity of the peritoneum, thereby maintaining optimal visibility within the operative field. Following confirmation of hemostasis, surgical specimens were extracted via a lower midline abdominal incision. A detailed animated representation of the full procedure is provided in Supplementary video and Supplementary video 2.
The TLRC technique employed in this study was consistent with approaches previously reported in the literatures[10, 11]. After establishing pneumoperitoneum via a periumbilical 10 mm port, four additional ports were inserted under direct vision. The peritoneal cavity was entered, and the sigmoid colon was mobilized to access the left ureter. The bladder and surrounding structures were dissected intraperitoneally. The peritoneum was routinely opened, and pelvic lymphadenectomy was performed. Urinary diversion was performed via the transperitoneal approach. All surgeries were performed by two senior urologic surgeons with more than 10 years of experience in laparoscopic radical cystectomy. To reduce potential variability and learning curve bias, both surgeons received structured training and jointly developed a standardized protocol before implementing the ELRC technique in clinical practice. Initially, TLRC was the standard approach, but as surgical proficiency and confidence with ELRC increased, the surgical team transitioned to ELRC as the preferred method. Both ELRC and TLRC procedures were distributed evenly between the two surgeons. All patients received perioperative care in accordance with standardized ERAS protocols.
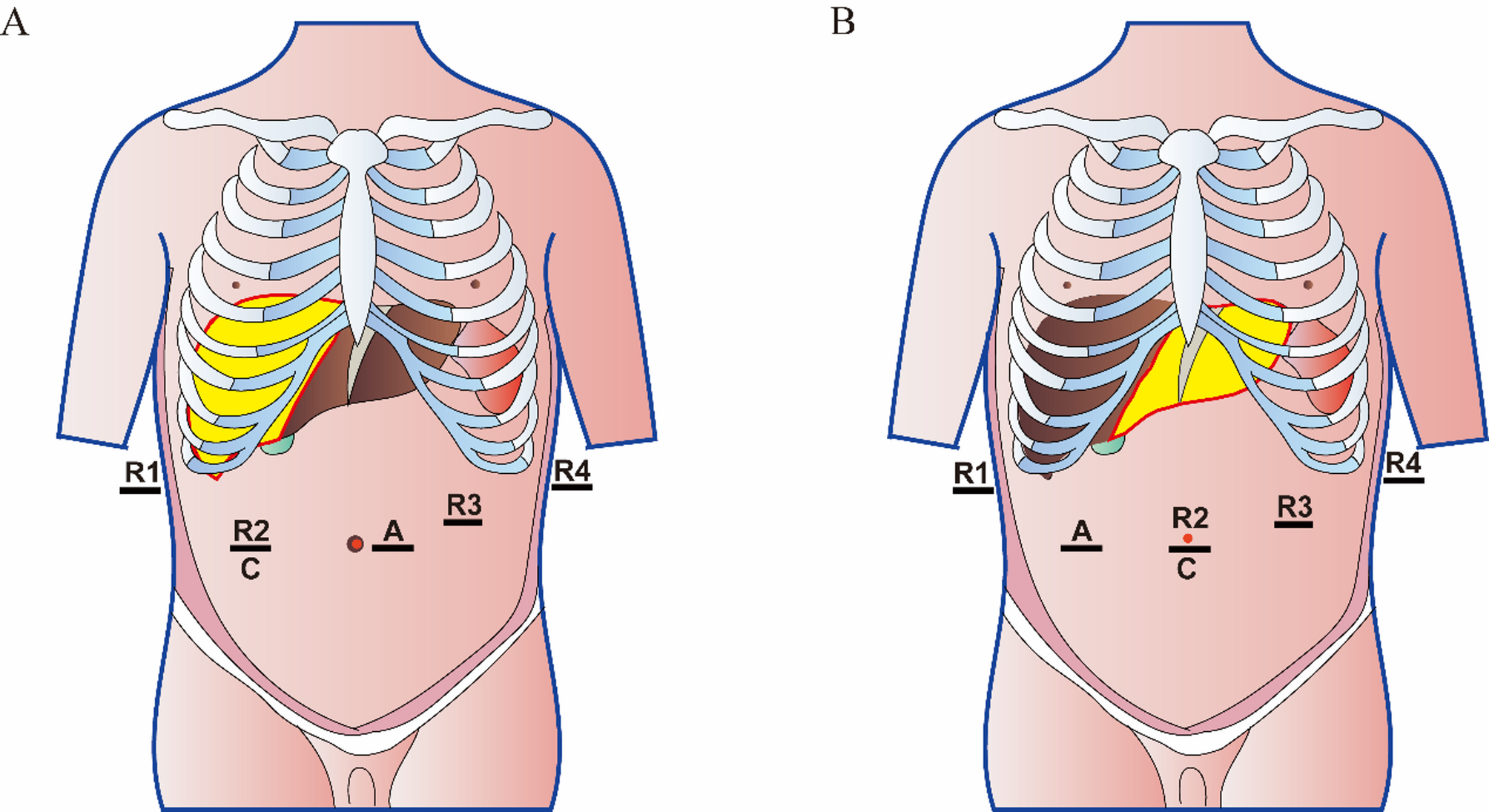
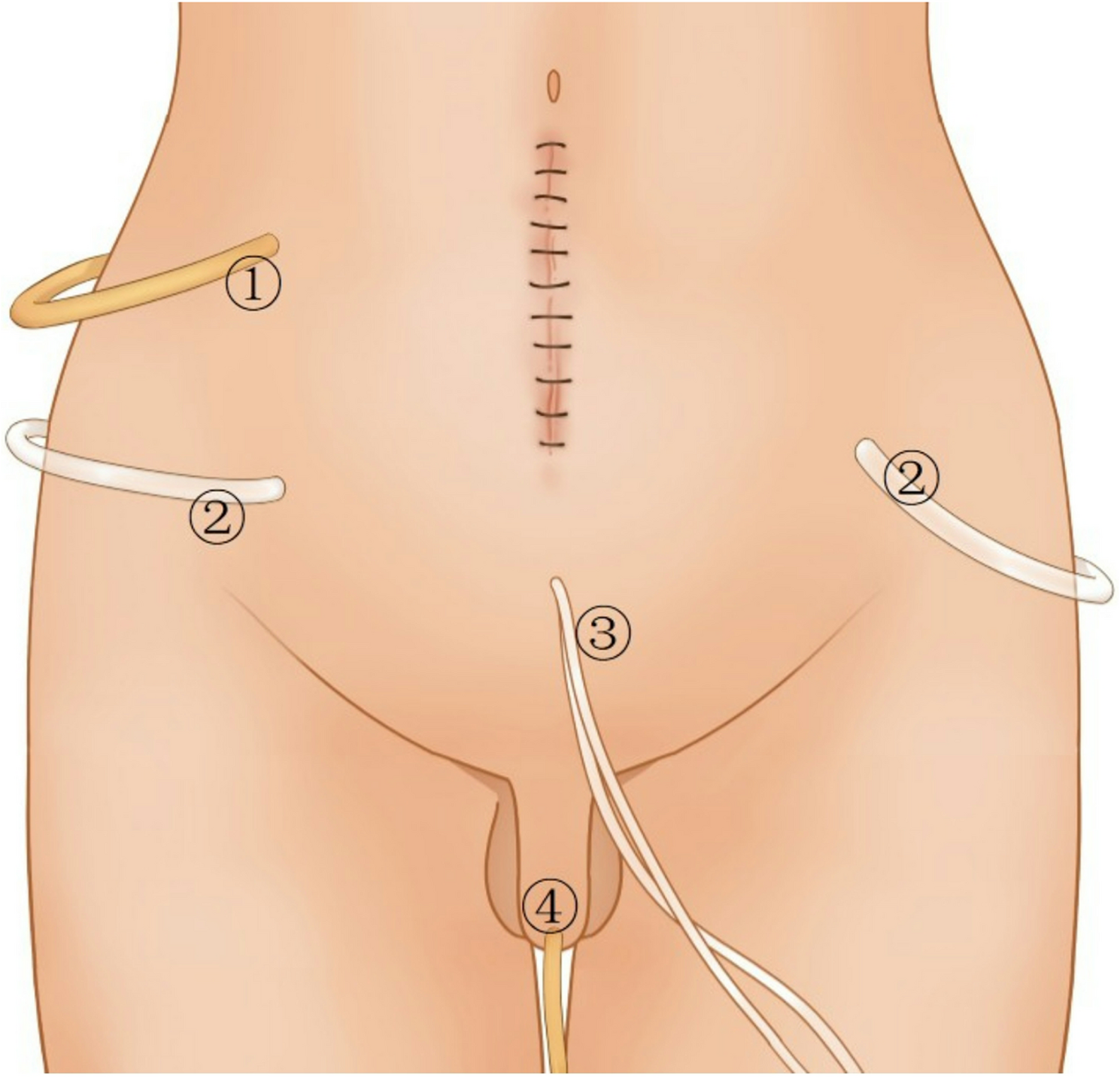
Postoperative managementAfter operation, parenteral nutrition was generally administered for the first 3 day. A small amount of water was allowed by oral intake at 24 h after surgery, which could improve intestinal function. Somatostatin was just used for one time after operation, if no ileus. Antibiotic prophylaxis was administered for 5 days after surgery. Cough, pounding back and blowing balloons were used for improving pulmonary function and nebulization was administered if necessary. Removal time of drains and catheter were illuminated in Fig. 1. Wound and drains should be kept clean and sterilized according to the need. Intraperitoneal drain would be removed from 4 to 7 days after operation. Extraperitoneal drains would be removed from 10 to 14 days after surgery (less than drainage fluid 30 ml per day for 3 days). 8. As for ION patients, Single-J stents would be removed for 1 month after surgery. The catheter was removed for 1week after single-J stents removal. As for ileal conduit patients, single-J stents would be removed for 1 month after surgery. For cutaneous ureterostomy patients, single-J stents would be replaced every 3–6 months.
Fig. 1
The position of drains and catheter after ELRC. 1 was the intraperitoneal drain, which should be removed for 5–7 day after operation. 2 were bilateral extraperitoneal negative pressure drains. One-sided negative pressure drain was removed first for 10 days after operation. Then the other side drain was removed another 3 days. 3 were single-J stents that was removed for 1 month after surgery. 4 was a catheter that was removed for 1 week after single-J stents removal. Drains were removed on condition of less than 30 ml drainage fluid per day for 3 days
Follow‑up and outcomeFollow-up was conducted every three months during the first two years after surgery and included computer tomography (CT) scan, physical examination, vital signs monitoring, routine blood and urine tests, and a standardized questionnaire for adverse events. CT urography (CTU) was repeated every six months. After two years, low-risk patients underwent annual CTU follow-up, while high-risk patients continued biannual CTU surveillance. This protocol was based on internal institutional policy rather than strict adherence to EAU or AUA guidelines. The primary endpoint of this study was overall survival (OS). Secondary endpoints included progression-free survival (PFS), cancer-specific survival (CSS), recurrence-free survival (RFS), and perioperative outcomes. Recurrence was defined as either local (within the surgical field) or distant. Disease progression was defined as lymph node involvement or distant metastasis. Urinary continence was evaluated at 1, 3, 6, and 12 months after surgery. Urinary continence outcomes were assessed only in patients undergoing ileal orthotopic neobladder reconstruction. Daytime continence was defined as the use of 0–1 pad per day. Nighttime continence was defined as ≤ 1 pad per night with no involuntary leakage during sleep. Continence status was determined through outpatient visits or structured telephone interviews using standardized follow-up questionnaires at 3, 6, and 12 months postoperatively. The assessment focused on patients who underwent ileal orthotopic neobladder reconstruction. Treatment-emergent adverse events (TEAEs) and serious adverse events (SAEs) were documented and evaluated both during hospitalization and follow-up using the Clavien-Dindo classification system [12]. Complications were graded according to the Clavien–Dindo classification system, with major complications defined as Grade III or above.
Statistical analysisThe statistical analysis was conducted utilizing R version 4.3.1 (R Foundation for Statistical Computing, Vienna, Austria) along with GraphPad Prism (GraphPad Software, San Diego, CA, USA). Continuous variable results were summarized either as means (with standard deviations [SD]) or medians (along with interquartile ranges [IQR]), based on the normality of the data evaluated through the Shapiro-Wilk test. Normally distributed data were compared using Student’s t-test; otherwise, the Mann–Whitney U test was employed. Categorical variables were compared using the χ² test or Fisher’s exact test, as appropriate. Kaplan-Meier analysis was utilized to estimate survival rates, while the log-rank test assessed differences between patient groups. The Cox proportional hazards regression model was employed to calculate hazard ratios (HR) and 95% confidence intervals (95% CIs) as well as for both uni- and multivariate survival analyses, adjusting for potential confounders including age, sex, ASA score, pathological T stage, urinary diversion type, and follow-up time. All statistical tests were two-sided, with a significance threshold set at P < 0.05.
Comments (0)