
Remember me



A retrospective analysis was conducted on patients who underwent open or robotic hepatectomy by the same surgical team at the First Affiliated Hospital of Guangxi Medical University from January 2021 to January 2024. Inclusion criteria were: (1) age > 18 years; (2) tumor diameter ≥ 5 cm; (3) no severe major organ dysfunction; (4) no history of other malignant tumors; (5) postoperative pathological diagnosis of HCC. Exclusion criteria were: (1) pathological diagnosis of other types of malignant tumors. (2) patients who received interventional, targeted, immunological, or radiotherapy treatments preoperatively.
This study was approved by the local ethics committee (approval number: 2024-E394-01). The study complies with the Declaration of Helsinki. All patients and their families were informed about the study and consented to participate.
Preoperative evaluationAll patients underwent routine clinical examinations, two imaging examinations (ultrasound, CT, or MRI), and laboratory tests, including total bilirubin, serum albumin, prothrombin time, international normalized ratio, alanine aminotransferase, aspartate aminotransferase, hepatitis B surface antigen, hepatitis C surface antibody, and tumor marker AFP. The diagnosis and treatment plan for each patient was determined by a multidisciplinary team. The choice between open and robotic hepatectomy depended on the patient’s condition and preferences, the surgeon’s expertise, the tumor’s size and location, and the availability of equipment. Preoperative data included gender, age, height, body mass index, American Society of Anesthesiologists classification, and key laboratory test results. Staging was determined using the Barcelona Clinic Liver Cancer (BCLC) staging system [11]. The extent of cirrhosis was assessed using the Ishak scoring system [12].
Surgical procedureFrom January 2021 to January 2024, our team performed a total of 221 robotic hepatectomy. All resections in this study were performed by two senior surgeons after completing their individual learning curves (≥ 60 robotic hepatectomy cases).
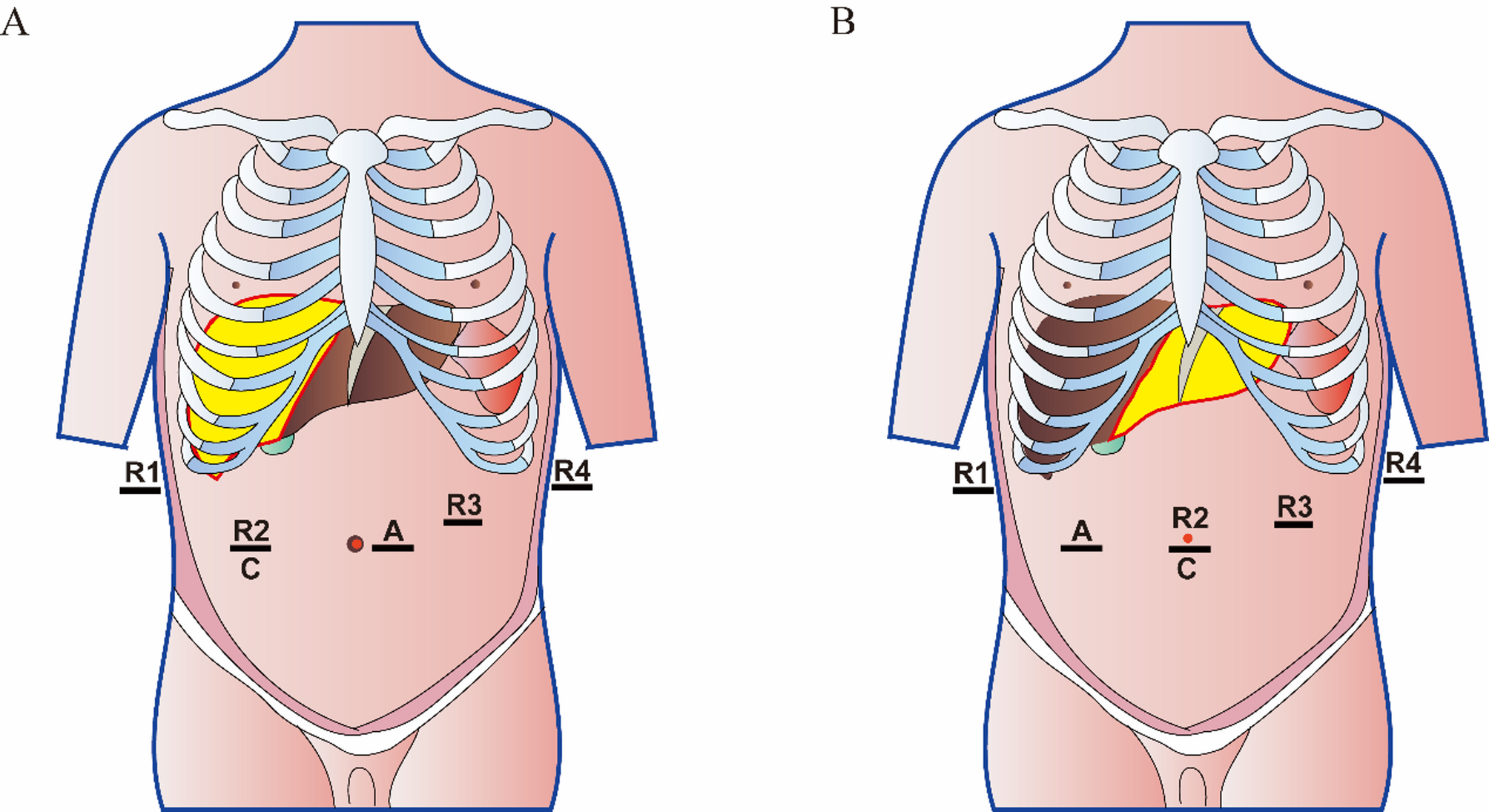
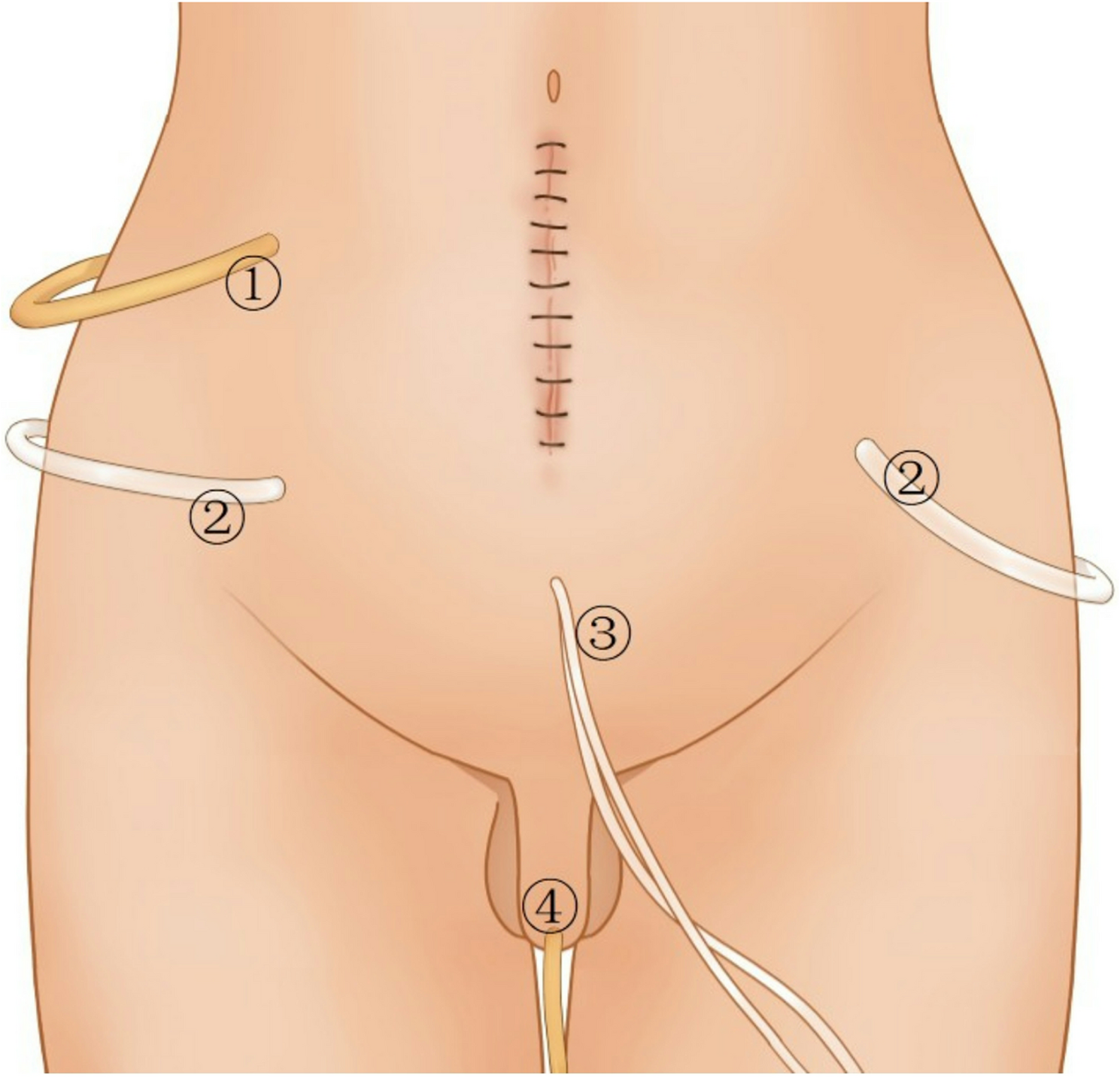
Anterior approach was used both in open and robotic hepatectomy. The systems used for patients undergoing robotic hepatectomy include the da Vinci Xi robot and the da Vinci Si robot. For right hemihepatectomy, a 12 mm trocar was placed at the umbilicus as the assistant’s operating port. The first and fourth robotic arms’ 8 mm trocars were positioned below the costal margin at the right and left anterior axillary lines, respectively. An 8 mm trocar for the third robotic arm was placed between the fourth robotic arm and the assistant’s port. A 12 mm trocar was positioned at the midpoint between the right anterior axillary line and the midline at the umbilical level as the camera port. The second robotic arms’ 8 mm trocars were positioned above the camera port (Fig. 1A). For left hemihepatectomy, a 12 mm trocar was placed at the umbilicus as the camera port. Another 12 mm trocar was positioned at the midpoint between the right anterior axillary line and the midline at the umbilical level as the assistant’s operating port. The first, second, and fourth robotic arms were positioned below the costal margin at the right anterior axillary line, at the camera port, and below the costal margin at the left anterior axillary line, respectively. The third robotic arm was positioned between the fourth robotic arm and the camera port (Fig. 1B). The anatomical separation during robotic right hemihepatectomy and left hemihepatectomy is shown in Fig. 2. Open liver resection surgery employs an anterior approach: a reverse L-shaped incision was used. The operational steps of the two methods are similar. Intraoperative ultrasound reassesses the tumor’s location, size, number, and positions of adjacent blood vessels, especially the anatomical relationships of the right, middle, and left hepatic veins. In right hemihepatectomy, cholecystectomy was performed firstly. The hepatic artery and portal vein were dissected individually and divided. Ultrasonic scalpel was used for liver parenchyma transection with low CVP. The Pringle maneuver is used, with intermittent clamping for 15 min followed by 5 min of reperfusion. The left/right hepatic vein was divided by surgical stapler. The specimen was removed. The surgical field was examined. Abdominal drainage was put in the surgical field.
Intraoperative data and pathological results were collected, including operative time, blood loss, transfusion status, tumor size, and vascular invasion. Intraoperative blood loss is calculated from the difference between fluid in the suction canister and abdominal irrigation fluid, plus the weight difference between surgical gauze and dry gauze [13]. Major vascular invasion is defined as the intrahepatic tumor invading branches of the portal vein or hepatic veins, and extrahepatic invasion of the portal vein trunk or inferior vena cava [14]. Microvascular invasion is defined as microscopic tumor invasion identified in the portal vein and hepatic veins of the surrounding liver tissue adjacent to the tumor edge. It refers to the presence of nests of cancer cells (≥ 50 cells) within endothelial cell-lined vascular lumens observed under a microscope [15, 16].
Fig. 1
The placement of the trocars in the da Vinci Xi robot system is illustrated in the figure. (A) Distribution of trocar positions for right hemihepatectomy. The yellow-marked area indicates the resection range. (B) Distribution of trocar positions for left hemihepatectomy. The yellow-marked area indicates the resection range
Fig. 2
Intraoperative demonstration of robotic right and left hemihepatectomy. (A) Separation of the right hepatic artery. (B) Separation of the right portal vein. (C) Isolation of the right hepatic duct. (D) Separation of the right hepatic vein. (E) Separation of the left hepatic artery. (F) Separation of the left portal vein. (G) Isolation of the left hepatic duct. (H) Separation of the left hepatic vein
Perioperative outcomes and long-term outcomesPerioperative outcomes included in the analysis are operative time, blood loss, postoperative stay, complications, and mortality. Postoperative stay is defined as the time from surgery to discharge. Postoperative complications included abdominal hemorrhage, bile leakage, ascites, liver failure, abdominal infection, and pulmonary complications. Abdominal hemorrhage is defined as a postoperative drop in hemoglobin greater than 3 g/dl from baseline and/or the need for transfusion or invasive reintervention to stop bleeding [17]. Bile leakage is defined as the bilirubin concentration in drainage fluid being three times or more the serum bilirubin concentration on or after the third postoperative day [18]. Ascites is defined as the drainage of more than 10 ml/kg of ascitic fluid per day from the abdominal drainage tube [19]. Postoperative liver failure is assessed using the 2011 criteria of the International Study Group of Liver Surgery (ISGLS) [20]. Abdominal infection is defined as the drainage of purulent fluid through the tube, isolation of organisms from sterile fluid or tissue cultures, or the development of abscesses or other evidence of organ space infection identified through direct examination, reoperation, histopathology, or imaging studies [21]. Routine CT scan is performed on the third postoperative day. Pulmonary complications include pneumonia, pleural effusion, atelectasis, and pulmonary embolism identified through CT scan [22]. The severity of postoperative complications is graded using the Clavien-Dindo classification, with Grade III and IV classified as major complications [23, 24].
Long-term outcomes included in the analysis are overall survival (OS) and disease-free survival (DFS). OS is defined as the time interval between surgery and death from any cause or the last follow-up. DFS is defined as the time interval between surgery and the first recorded tumor recurrence. All patients were followed up after discharge, with follow-ups every 3 months during the first year, and every 3 to 6 months thereafter. Routine examinations at each follow-up included complete blood count, liver function tests, tumor markers, immune test, and abdominal ultrasound. CT or MRI was performed if necessary. Recurrence was defined as the appearance of any new intrahepatic or extrahepatic tumor lesions on CT or MRI after hepatectomy. Post-recurrence treatments were selected based on the patient’s condition and individual preferences, and included surgical resection, radiofrequency ablation and microwave ablation, transarterial chemoembolization (TACE), or systemic therapy. The last follow-up was on May 1, 2024.
Statistical analysisCategorical variables are presented as numbers and percentages, while continuous variables are presented as medians and interquartile ranges. Continuous variables were compared using the Mann-Whitney U test, and categorical variables using the Chi-square test or Fisher’s exact test. Propensity score matching (PSM) was used to eliminate selection bias between the two groups. PSM analysis was performed using a 1:1 ratio based on the nearest neighbor matching method with a caliper set to 0.20. Constructed using a logistic regression model incorporating age, sex, body mass index (BMI), albumin, total bilirubin, platelet, alanine aminotransferase(ALT), aspartate aminotransferase(AST), international normalized ratio(INR), serum α-fetoprotein(AFP), viral hepatitis infection, Child-Pugh grade, Barcelona Clinic Liver Cancer (BCLC) stage, indocyanine green retention rate at 15 min(ICG15), portal hypertension, model for end-stage liver disease (MELD) score, tumor number, tumor size, vascular invasion, and American Society of Anesthesiologists (ASA) classification. Kaplan-Meier (KM) curves were used to analyze OS and DFS, with comparisons made using the log-rank test. A p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 26.0.
Comments (0)