The current study evaluated the clinicopathologic characteristics and predictors of treatment failure of patients with clinically evident metastatic PTC to the lateral neck (N1b). The highest rate of lymph nodes metastasis in the lateral neck was found at level III, followed by levels IV and II. However, for about 77% of the patients with lateral neck metastases, the metastatic disease was also in the central neck. Similar findings were reported by Chinn and others [17,18,19]. On the contrary, Huang et al. reported the highest rate of metastases at level IV, in the lateral neck, followed by level III [20]. Among our patients, lymph nodes metastasis presented in 55% of the level II dissections. This finding supports dissection of level II in metastatic papillary carcinoma to the lateral neck. Song et al. suggested a super-selective lateral ND, including levels III-IV, in patients with PTC, when the preoperative evaluation identifies a single lymph nodes metastasis located at levels III-IV and the primary tumor is not in the upper lobe of the ipsilateral thyroid [21].
Due to the high rate of injury of the spinal accessory nerve while dissecting level V, and the low rate of occult metastasis, we currently dissect level V only in the presence of pathological LN on imaging (especially ultrasound). Despite avoiding dissection of level V, we found no increase in treatment failure in patients with metastasis at this level. Other studies support the same strategy [21, 22].
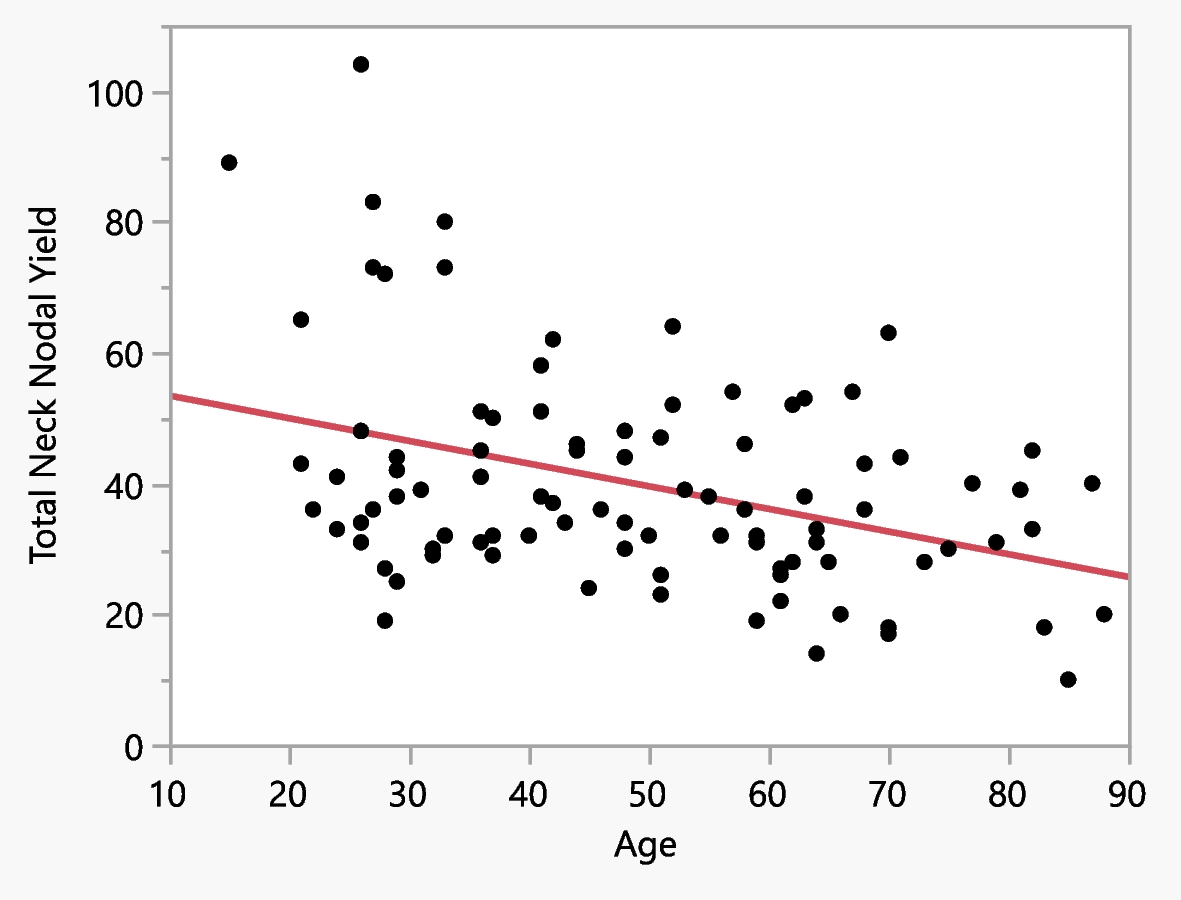
Our study showed a significant inverse correlation between patients' age and total NY. The number of LN removed in ND was higher in our younger than older patients. To the best of our knowledge, such a significant linear regression model was not reported in the literature, although an inverse correlation was previously published between age and NY [13].
In addition to the above, we found a significant inverse correlation between patients' age and the number of positive neck lymph nodes metastasis. Among younger patients, the mean number of metastatic nodes was higher. A number of studies have identified young age as a risk factor for lymph nodes metastasis and prognosis [5, 13, 23, 24]. However, we are not aware of reports of an inverse correlation in a linear regression model like ours, between age and the number of positive lymph nodes metastasis.
Twenty patients (21%) had treatment failure, either recurrence (11 patients) or persistent disease (9 patients). Of eleven patients (11%) who had recurrence, four had recurrences in the central neck and five in the ipsilateral neck, which was previously operated. Other studies reported recurrence rates between 16 and 43% [4, 5, 8, 25].
Parameters that were significantly associated with treatment failure were patient age, positive tumor margins, lympho-vascular invasion, the total number of positive nodes, and nodal ECE. In multivariate analysis, the independent predictors for treatment failure were patient age, positive tumor margins, the total number of positive nodes in ND, and nodal ECE.
The association between patient age and treatment failure is inconclusive. Some studies presented a significant correlation between them [5, 12, 13, 26, 27] while other did not [8, 10]. The current study found a significant correlation of age to treatment failure and recurrence-free survival. As age was inversely correlated with the total NY and the number of positive LNs, it was associated with LNR. Therefore, after adjusting for age in multivariate analysis, the association of LNR with treatment failure was found to be non-significant.
The presence of positive tumor margins was identified as a significant predictor of treatment failure. We are not aware of any study that found positive tumor/ surgical margins as a prognostic parameter. However, our finding of a high correlation of positive margins with ETE might explain the higher rate of failure in these patients. Carmel Neiderman et al. found that positive resection margins were non-significant predictor for recurrence [13].
The number of metastatic nodes and nodal ECE were also identified as significant prognostic factors of PTC in a number of studies [2, 13, 15, 28, 29]. According to Randolph et al., these parameters were associated with recurrence but not with OS [28]. Sappupo et al. reported that the number of LNM was associated with a worse outcome (persistent/ recurrent disease) when > 5 metastatic LNs were present in the central neck (N1a), but not when present in the lateral neck (N1b) [15].
We report no significant correlations of treatment failure with gender, primary tumor size, multifocality, size of the greatest positive node, NY, and LNR. These findings contrast with studies that published associations of these parameters with disease recurrence [4, 8, 10, 14, 25,26,27, 30, 31].
We found that the number of metastatic nodes, rather than LNR, was a significant predictor of DSS. Five-year DSS and OS were 96% and 93%, respectively, and 10-year DSS and OS were 85% and 78% for all T stages. These rates are consistent with the data in the literature [9, 13, 30, 32]. DSS was correlated to patients’ age, the size of the primary tumor and the number of LNM found in ND. However, among patients younger than age 55 years compared to older patients, 5-year and 10-year DSS and OS rates were significantly higher: 100% Vs 89% (DSS) and 100% vs. 86% (OS) and 100% Vs 48% (DSS) and 100% vs. 45%(OS), respectively. Indeed, only one patient in the younger group died of other causes, at age 41 years.
The age cutoff of 55 years for staging PTC was published in the American Joint Committee on Cancer, 8th edition [33]. Patients older than 55 years were shown to have worse outcomes [13, 33, 34]. The only predictive factor for overall survival in the current study was patient’s age. Among patients aged > 55 years compared to younger patients, the rate was higher of tumor multifocality; and the rates were lower of total NY, the number of positive nodes, and LNR. Importantly, among the older compared to the younger patients, treatment failures were more common (32% vs. 13%), the mean thyroglobulin level was higher, and the outcomes were worse.
Similar to our findings, Carmel Neiderman et al. reported higher total NY, metastatic nodes, and LNR, among patients younger than age 55 years compared to older patients [13]. Cancer et al. reported higher OS and disease-specific survival rates among patients < 50 years [7]. However, in contrast to our results, they found regional recurrence in a higher proportion of this group.
Amit and others found LNR to be an independent predictor for disease-specific survival and OS, in addition to the following parameters: sex, age, the presence of distant metastasis, nodal ECE, and RAI treatment [6, 9]. We believe that as patient's age affects the number of positive nodes and the NY (and therefore the LNR), it affects DSS and OS more than does LNR by itself. Although the total dose of RAI was found to be significantly correlated to treatment failure, we assume that this is the result of treatment failure rather than a predictor to failure. Patients who had recurrent disease received second and third doses of RAI.
Other studies identified age and tumor size as predictors of mortality [9, 31, 35, 36]. Importantly, both factors have been suggested as parameters that define active surveillance in thyroid cancer [32]. According to Robinson et al., the probability of occult nodal disease affects OS at all tumor stages [11]. Sapuppo et al. published N1b stage by itself is a risk factor for distant metastasis and cancer-related death [37]. The retrospective single-center design and relatively small sample size are limitations of the study. In addition, due to the low mortality rate of patients aged ≤ 55 years, we could not analyze prognostic parameters that affect OS for this group.




Comments (0)