This study confirmed that the balloon method outperformed the gauze packing method in terms of shape reproducibility and procedural efficiency. Specifically, the balloon method enabled the application of uniform pressure within the vaginal cavity, allowing for precise replication of its shape. As a result, the accuracy of radiation delivery in intracavitary brachytherapy can be improved, potentially maximizing therapeutic efficacy. Furthermore, the shorter procedural time achieved with the balloon method suggests improved treatment efficiency. Gauze packing is commonly used in ICBT with tandem and ovoid applicators. Investigating the use of balloons as an alternative to gauze packing have reported that the balloon packing method provides greater patient comfort [6, 7]. Although references [5,6,7] primarily discuss packing methods in the context of tandem and ovoid or ring applicators, the findings related to patient comfort and cavity filling uniformity remain conceptually relevant to vaginal mold preparation, and support the rationale for exploring alternative packing techniques such as balloon-based methods. In pediatric vaginal rhabdomyosarcoma cases, standard cylindrical applicators are not suitable due to their size. However, the balloon method proposed in this study may offer a viable alternative for these cases, providing more accurate cavity shaping while minimizing discomfort. This approach could potentially be applied in pediatric cases, where conventional methods are challenging, as demonstrated in other studies [10].
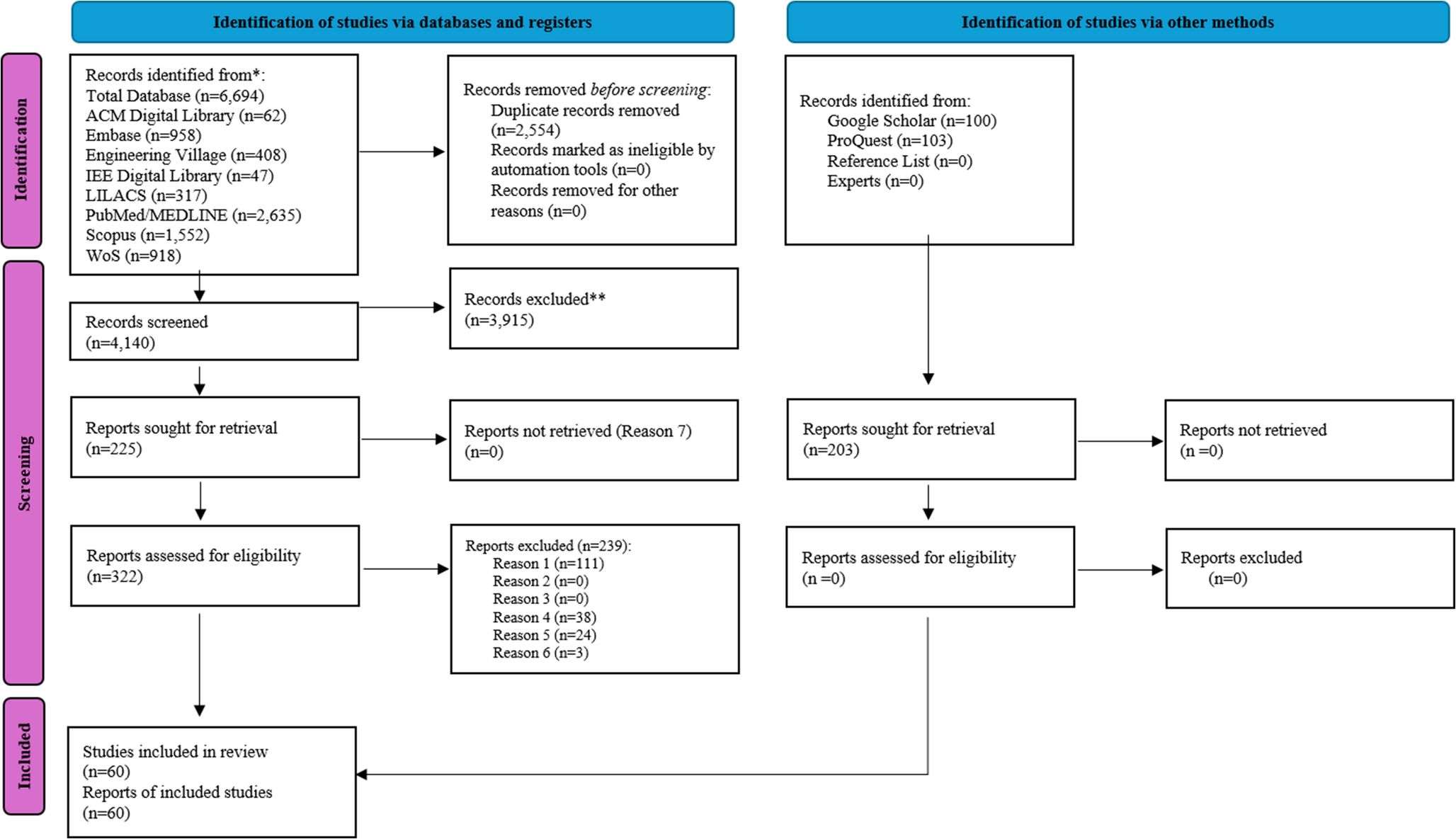
The gauze packing method might fail to achieve uniform distribution of gauze within the vaginal cavity, as illustrated in Fig. 3, resulting in uneven filling. This unevenness compromises the accuracy of custom-made cylinders, increasing the risk of reduced precision during intracavitary brachytherapy. For patients with irregular vaginal morphology or adhesions along the vaginal walls, incomplete gauze distribution exacerbates the difficulty of achieving precise shape replication. Such inconsistencies can adversely affect radiation delivery, potentially diminishing rather than enhancing therapeutic effects.
Additionally, the vaginal model used in this study features complex structures such as the “dog-ear” shape of the vaginal apex formed by the external cervical os and vaginal fornices, resembling real vaginal morphology [4, 11]. The balloon method successfully conformed to these complex shapes, as demonstrated in this study. While previous methods have struggled to deliver sufficient doses to the vaginal apex, our balloon method enables accurate replication of vaginal morphology and adaptation to intricate shapes. This finding supports the versatility of the balloon method and its potential applicability to other vaginal models with varied shapes. Previous studies have reported that balloon packing can improve patient comfort and provide more reproducible cavity shaping compared to gauze packing [6, 7]. Consistent with this trend, our results demonstrated reliable cavity conformation and a reduction in procedural time, underscoring the practical advantages of the balloon-based approach. Furthermore, recent studies employing customizable molds for pediatric patients [10] and complex vaginal anatomies [11] emphasize the growing clinical demand for adaptable cavity-shaping techniques—an area to which our method offers a promising contribution.
However, this study has several limitations. The vaginal model used was designed to simulate general vaginal morphology but does not account for individual variations in tissue elasticity and hardness. Further studies are needed to evaluate the effectiveness of the balloon method in accommodating the diverse vaginal morphologies of actual patients. Moreover, the study focused primarily on shape uniformity and procedural time, without directly assessing the impact on radiation dose distribution or clinical outcomes. In addition, shape uniformity was evaluated qualitatively on CT images; quantitative metrics such as volume deviation or surface-to-surface error were not calculated, and should be incorporated in future investigations.
Future investigations should include dosimetric analyses and patient-reported outcomes to provide a more comprehensive evaluation. Additionally, this study did not include any in vivo validation, and the findings are based solely on simulations using a synthetic vaginal model. While the SD TENGA model was selected for its anatomical resemblance and structural complexity, it does not fully replicate the biomechanical properties of human vaginal tissue, such as elasticity, compliance, or dynamic pressure response. Therefore, further validation using patient-specific data or animal models may be necessary to confirm the clinical applicability of the balloon method. This study focused on developing a balloon-based method for vaginal cavity molding; however, the obtained cavity data can serve as a foundation for fabricating applicators with pre-defined source channels. Future implementation may involve creating a negative mold from the cavity shape and embedding catheters or source paths prior to casting with biocompatible materials such as silicone, enabling customized dose delivery to HR-CTV or target surfaces.


Comments (0)