
Remember me
From 2009 to 2025 we treated 235 patients with one or multiple infratentorial brain metastases by surgery. Sex was nearly equally distributed; 122 patients were female, 113 were male. Median age was 66 years (IQR 56–74). Cancer type was lung in 83 patients (35.32%), breast in 49 patients (20.85%), melanoma in 14 patients (5.96%), CUP in 5 patients (2.13%), GIT in 42 patients (17.87%), RCC in 8 patients (3.40%), urothelial carcinoma in 6 patients (2.55%) or others in 27 patients (11.49%). Rate of preoperative hydrocephalus was 34.62% and of persisting postoperative hydrocephalus was 18.38%.
Epidemiological, preoperative and postoperative clinical data as per cancer type are depicted in Table 1a–c.
Table 1 Epidemiological (a), preoperative (b) and postoperative (c), clinical data per cancer typeLooking for significant differences in epidemiological and clinical data of the cancer types we performed an ANOVA with post-hoc correction for age, tumor volume and time from diagnosis to death. While age was statistically significant (p = 0.0343) post-hoc correction showed none of the pairwise differences were large enough to reach significance after correction. There was no statistically significant difference in tumor volume or time from diagnosis to death.
Comparing all binary variables between cancer types we found almost no statistically significant differences after performing multiple Fisher’s exact tests with Bonferroni correction (Table 1). The only significant parameter was proportion of female sex as 100% of patients with breast cancer were female.
Data analyses at primary endpointPostoperative hydrocephalus was reported in 43 of 235 patients (18.45%). The rate of postoperative hydrocephalus was highest in breast cancer (30.61%) and lowest in CUP and urothelial carcinoma in which no cases of postoperative hydrocephalus were reported (Table 1). Comparing breast cancer to the other cancer types in which postoperative hydrocephalus was found, there was a significant difference compared to most common type, lung cancer (15.66% vs. 30.61%; p = 0.042). Preoperative hydrocephalus did significantly correlate with postoperative hydrocephalus over all cancer types (p = 0.005) while acute presentation did also correlate with preoperative hydrocephalus (p = 0.014).
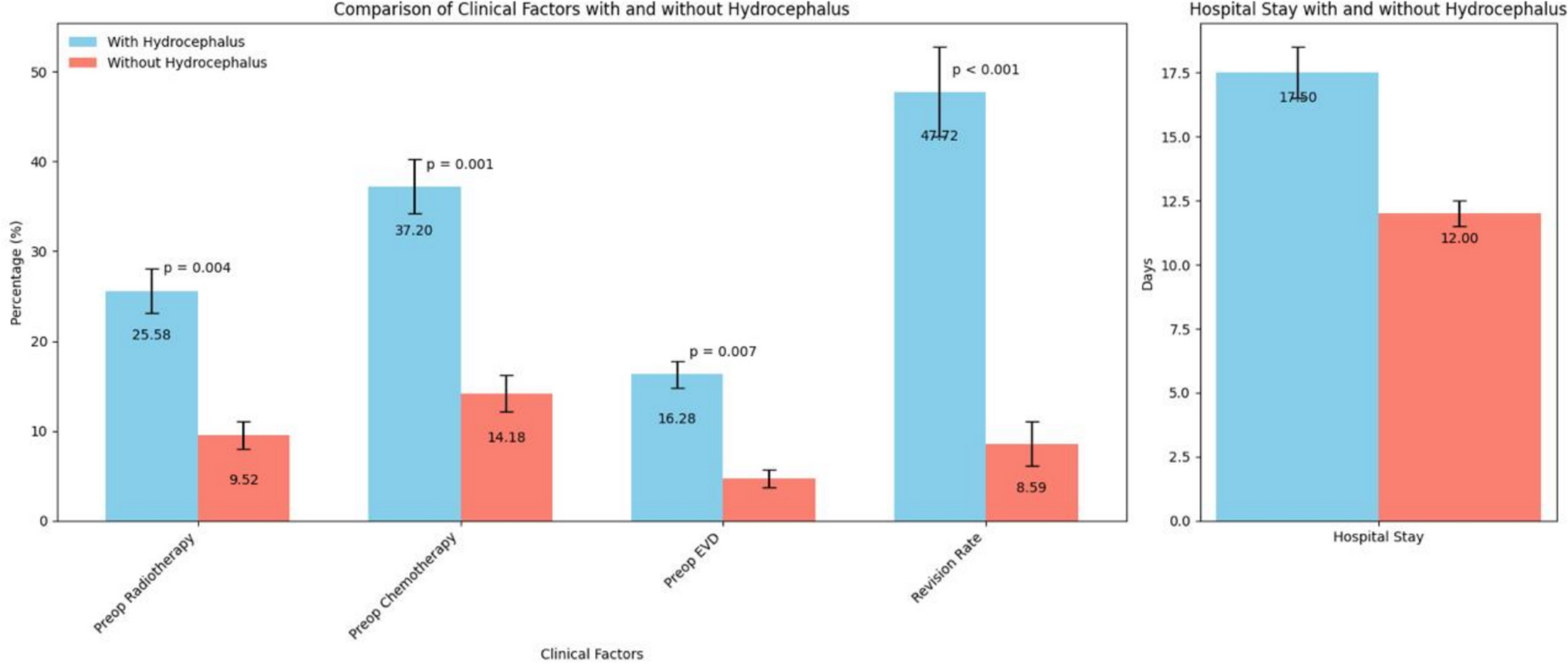
Comparing patients with postoperative hydrocephalus to patients without postoperative hydrocephalus there was no significant difference in age (65.65 vs. 64.80 years; p = 0.687), tumor volume (12.39 ml3 vs. 15.12 ml3; p = 0.130), proportion of female sex (62.79% vs. 50.00%; p = 0.131) or rate of complete resection (69.77% vs. 85.55% (p = 0.564). Significant differences were found in patients treated with preoperative radiotherapy (25.58% vs. 9.52%; p = 0.004) or preoperative chemotherapy (37.20% vs. 14.18%; p = 0.001), and in patients with preoperative EVD (16.28% vs. 4.73%; p = 0.007). Furthermore, there was a significant difference in revision rate for patients with and patients without postoperative hydrocephalus (47.72% vs. 8.59%; p < 0.001) as well as in length of hospital stay (17.50 days vs. 12 days; p < 0.001) (Fig. 1). Revision surgery was performed following postoperative bleeding in 38.10%, posterior fossa swelling in 14.30%, infection in 19.04% and active CSF leakage in 28.57%.
Fig. 1
Comparison of relevant independent clinical variables in patients with and without postoperative hydrocephalus
Sub cohort analyses of patients with early onset hydrocephalus and late onset hydrocephalus without prior EVD placement revealed that there were no differences in age, proportion of female sex, tumor volume, preoperative radiotherapy, or preoperative chemotherapy.
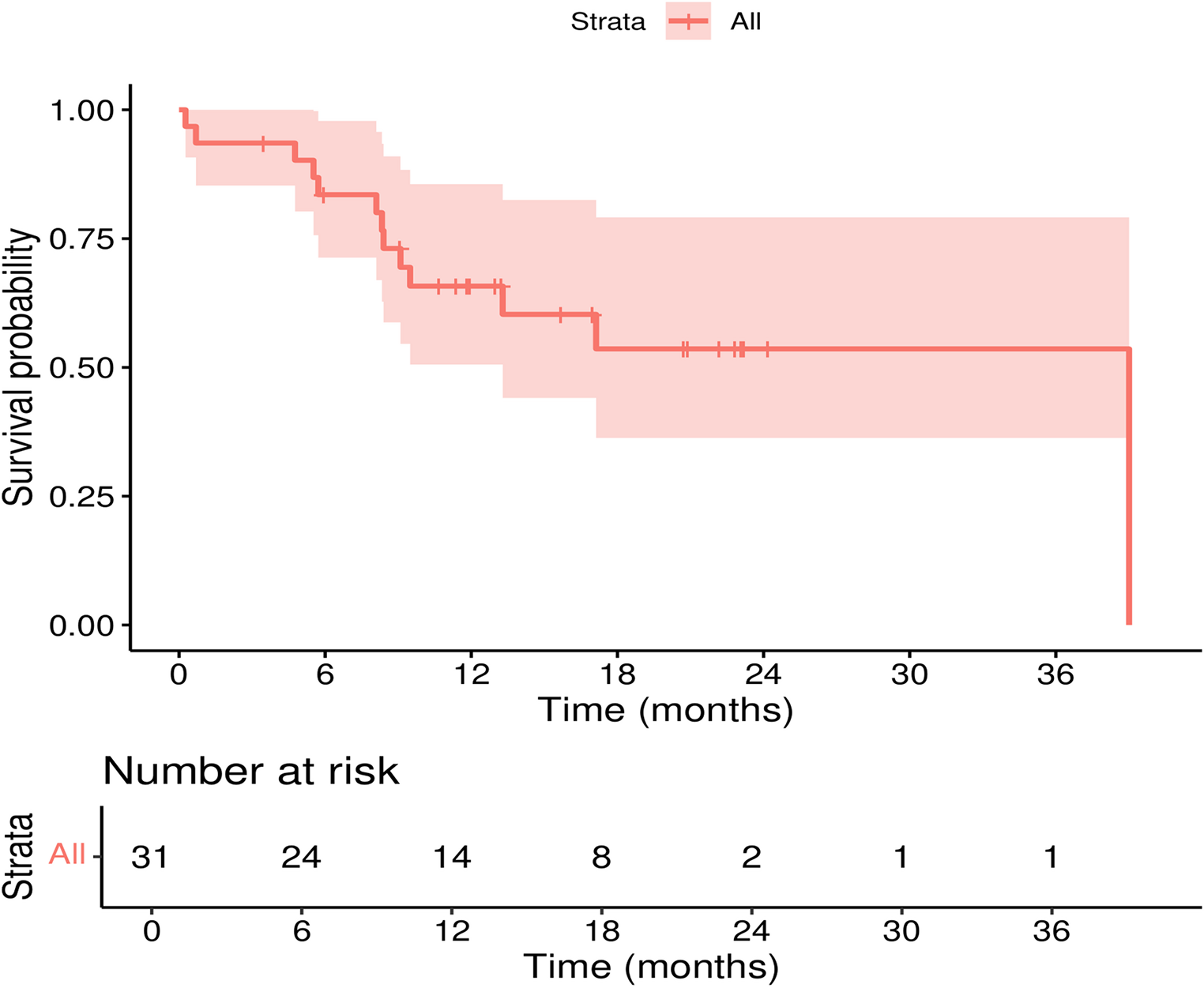
Survival analysesMedian survival in patients with postoperative hydrocephalus was 5 months (95% C.I. = 3–13) and 16 months (95% C.I. = 14–26) in patients without postoperative hydrocephalus. There was a significant difference (p = 0.016) (Fig. 2a).
Fig. 2
Kaplan–Meier curves of patients with and without postoperative hydrocephalus (a) and of all patients grouped by cancer type regardless of hydrocephalus diagnosis (b) Median survival time is given in months
Grouped by cancer type there was no significant difference in median survival (p = 0.130) (Fig. 2b). Median survival ranged from 4 months (95% C.I. = 2–4) in other cancer types to 47 months (95% C.I. = 24–47) in urothelial cancer.
Prediction modelsTo look for independent predicting factors of postoperative hydrocephalus we first performed simple logistic regression analyses (Table 2). Statistically significant variables were preoperative hydrocephalus (p = 0.006), preoperative EVD (p = 0.011), preoperative radiotherapy (p = 0.006) and preoperative chemotherapy (p = 0.001).
Table 2 Simple regression analyses of relevant variables over all cancer types for data set explorationNext, we performed multiple regression analyses strictly accounting for sex and age. Variables were grouped in clinical (Table 3a), therapeutic (Table 3b) and imaging variables (Table 3c). Regarding clinical variables at first presentation, we identified preoperative hydrocephalus (p = 0.013) and acute presentation (p = 0.031) as significant predictors. In this scenario sex was also statistically significant (p = 0.022).
Table 3 Multiple regression analyses of relevant variables over all cancer types grouped into clinical (a), therapeutic (b) and imaging variables (c)Accounting for preoperative forms of cancer treatment radiotherapy (p = 0.032) and chemotherapy (p = 0.008) were found to be statistically significant predictors.
Imaging variables such as tumor volume, tumor location near the fourth ventricle or the occurrence of multiple infratentorial metastases were not found to be statistically significant predictors.
No evidence of multicollinearity was found among the independent variables, as all variance inflation factor (VIF) values were below 10 (Table 4).
Table 4 Multicollinearity analysis
Comments (0)