This is a Health Insurance Portability and Accountability Act-compliant, Institutional Review Board-approved prospective cohort study conducted at a comprehensive cancer center between September 1, 2019, and September 31, 2021 (Protocol Number 2018 − 0869). Eligible patients undergoing care at our institute were approached by the clinical or research staff to obtain written informed consent prior to enrollment.
Participants enrollment
Patients included in this study (1) were at least 18 years of age, (2) had a clinically suspected or biopsy-confirmed diagnosis of glioblastoma, isocitrate dehydrogenase-wildtype, and (3) were candidates for standard-of-care maximal safe tumor resection and adjuvant chemoradiation as determined by a multidisciplinary team of neuro-oncologists, neurosurgeons, radiation oncologists and neuroradiologists. Patients were excluded if they (1) were pregnant, (2) had a known allergy to gadolinium-based contrast agents or 18 F-Fluciclovine, (3) renal failure as evidenced by an eGFR less than 60 mL/min/1.73m2, or (4) pacemakers, electronic stimulation, metallic foreign bodies, and devices and/or other conditions deemed not MRI safe. Patients were also excluded (5) if histopathologic examination of resected tumor did not reveal high-grade histologic features such as central necrosis or microvascular proliferation. A total of 8 participants were enrolled in this study, which was substantially lower than the recruitment target of 25 patients due to the unexpected cessation of 18 F-Fluciclovine radiopharmaceutical distribution and the COVID-19 pandemic. The median follow-up time was 591 days (interquartile range 282–998). The ensuing article adheres to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist for cohort studies (Table S1, Online Resource) [16].
Clinical and histo-molecular data
Basic demographic characteristics such as age, sex, Karnofsky Performance Status at diagnosis; histo-molecular data including histologic grade, O6-methylguanine-DNA methyltransferase promoter (MGMTp) methylation status and EGFR amplification status; extent of resection reported by board-certified neuroradiologists at our institute on standard-of-care early postoperative MRI, within 48–72 h of surgery; [15] and cumulative radiotherapy dose were collected throughout the follow-up period. Overall survival (OS) was assessed from the date of preoperative MRI to the date of death or right-censoring.
Clinical imagingTimeline
Participants underwent serial MRIs and 18 F-Fluciclovine PET/CTs of the brain at four timepoints throughout disease course: (1) within 14 days prior to initial tumor resection i.e. at the preoperative timepoint, (2) within 7 days prior to initiation of radiation therapy i.e. at the pre-radiation timepoint, (3) within 28 ± 5 days following radiation therapy completion i.e. at the early post-radiation timepoint, (4) at 6 months ± 14 days following radiation therapy completion i.e. at the late post-radiation timepoint. All MRI and 18 F-Fluciclovine PET/CT scans were completed within 3 days of one another.
MRI acquisition
MRI scans were performed on a 3T clinical scanner (MR750, GE Healthcare, Milwaukee, WI, USA) using an 8-channel brain coil. Images from a 3D T2-weighted FLAIR sequence and a 3D T1-weighted GRE sequence acquired before and after contrast administration of 0.1 mmol/kg gadobutrol (Gadavist, Bayer HealthCare), respectively, were used for this study. The 3D FLAIR sequence was acquired as sagittal slices (TR = 7,000 ms, TR = 89 ms, TI = 2,069 ms, echo train length = 140, in-plane resolution = 1.1 mm x 1.1 mm, slice thickness = 0.5 mm with 50% resolution), and reformatted to 1.1-mm slices in the axial and coronal planes. The 3D GRE sequence was acquired as axial slices (TR = 5.8 ms, TE = 2.5 ms, flip angle = 20°, in-plane resolution = 1.1 mm x 1.0 mm, slice thickness = 0.7 mm with 50% resolution), and reformatted to 1.1-mm slices in the sagittal and coronal planes.
18 F-fluciclovine PET/CT acquisition and reconstruction
All patients were administered 5 ± 15 mCi of 18 F-Fluciclovine intravenously. Following 3 to 5 min in a quiet room, all patients were positioned supine on a GE Discovery 690 PET/CT system with arms next to their body. Position aids and warm blankets were used to ensure patient comfort during the scan time. Patient imaging then followed and consisted of a CT scout of the whole head, a CT scan for anatomical landmarking and attenuation correction, and a PET scan consisting of one bed position. The total scan time including patient positioning, radiotracer injection, CT and PET acquisition was about 45 min. The CT acquisition parameters were 120 kVp, with 0.5 s rotation, a pitch of 0.984, 3.75 mm slice thickness with 3.27 mm interval, and a 40 mm beam collimation (0.625 × 64). Tube current modulation was utilized to minimize patient radiation exposure. The CT data was then reconstructed with 512 matrix with a standard filter using a 25 cm FOV. The PET data, on the other hand, was acquired in 30 min with TOF and reconstructed using OSEM with 2 iterations and 32 subsets with a 6.4 mm gaussian filter and point spread function modeling using a 256 matrix and a 25 cm FOV. All PET data correction for attenuation, scatter, and randoms were applied during image reconstruction using manufacturer software on the scanner console.
Volumetric data
Tumor volumes on T1C, FLAIR and 18 F-Fluciclovine PET/CT were delineated using MIM software version 7.2 (MIM Software Inc., Cleveland, OH).
First, a research fellow manually segmented tumors on T1C and FLAIR. Enhancing blood vessels, venous sinuses, meninges, and areas of intrinsic T1 shortening, if any, were manually excluded from the T1C volume (T1CV) after careful examination of pre-contrast T1-weighted sequences. Areas of necrosis were included in the preoperative T1CV, consistent with previously published segmentation approaches [17], as necrotic burden has been shown to significantly correlate with survival in glioblastoma [18, 19]. Postoperative contrast enhancement about the surgical tract and resection cavity, along with the cavity itself were also excluded from the T1CV as well as the FLAIR volume (FLAIRV) to ensure accurate quantification of residual or recurrent tumor burden. Final contours were audited by a board-certified neuroradiologist to enhance accuracy and minimize interobserver variability, with only minor adjustments performed.
Independently, a second research fellow, blinded to the information provided by the anatomic MRI sequences, contoured the metabolically active tumors on 18 F-Fluciclovine PET/CT to derive the biological tumor volume (BTV) using the PETEdge + tool of MIM. This tool does not rely on a fixed uptake threshold or tumor-to-background ratio; it rather relies on a validated gradient approach that calculates spatial derivatives along tumor radii, then defines the tumor edge on the basis of derivative levels and continuity [20, 21]. This tumor mask was subsequently mirrored onto the contralateral normal appearing brain, and standardized uptake values of the tumor and background were derived. Final contours were reviewed by a board-certified neuroradiologist with experience in nuclear imaging with only minor adjustments performed.
Radiation target volume delineation
Radiation planning volumes were independently defined as gross tumor volume, clinical tumor volume and planning target volume. The institutional approach for glioblastoma contours is such that the gross tumor volume includes the resection cavity, the T1CV and portions of the FLAIRV if considered grossly abnormal. The clinical tumor volume is a 2 cm expansion from the gross tumor volume to encompass all FLAIR changes. Furthermore, the planning target volume margins are 3 mm with image-guided radiation therapy. Treatment planning is a two-volume simultaneously integrated boost approach with prescription dose of the gross tumor volume to 60 Gy and the clinical tumor volume to 50 Gy.
Statistical analysis
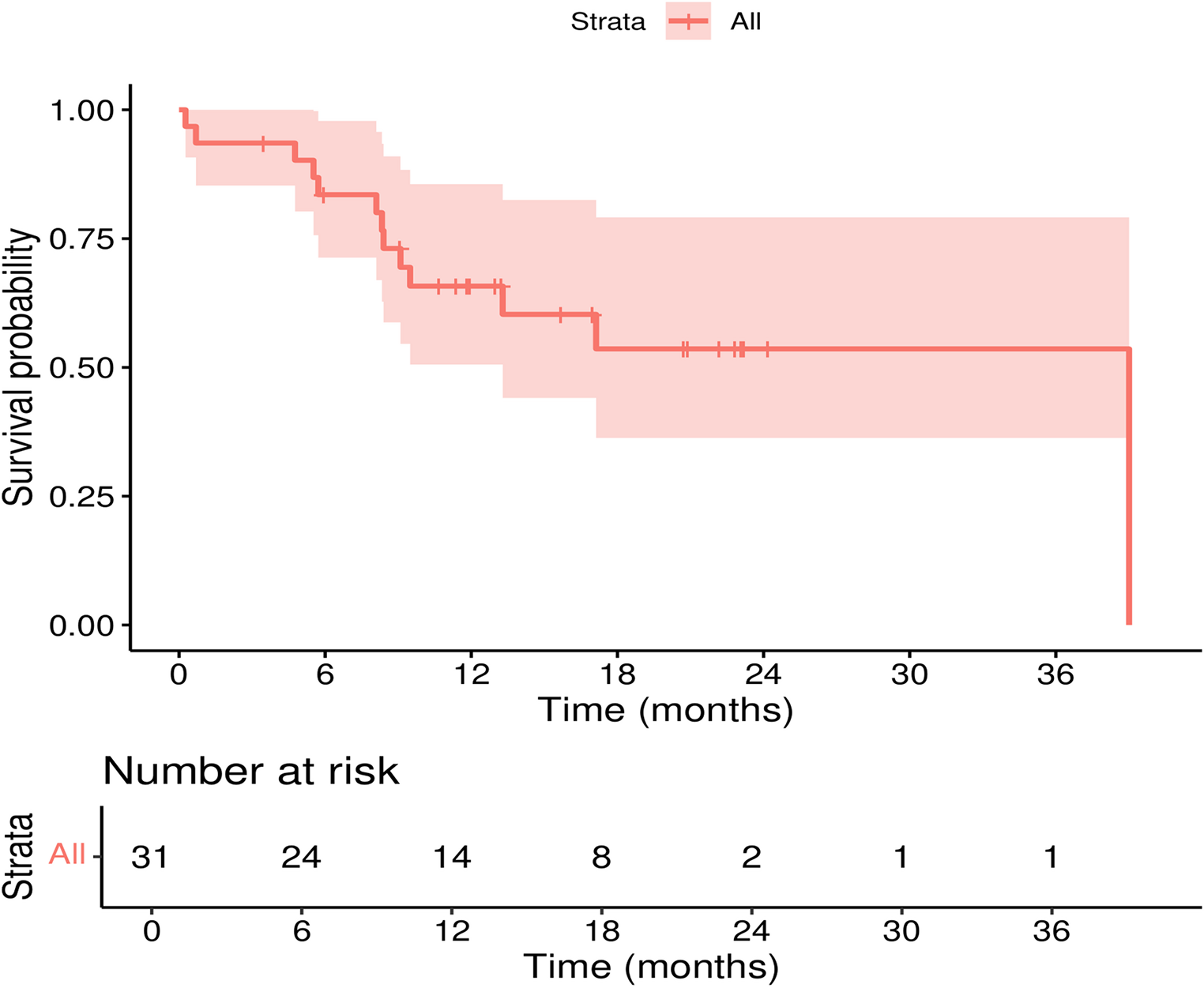
Data was analyzed with SPSS version 29.0 (IBM SPSS, inc., Chicago, IL). Qualitative and quantitative variables were summarized as frequency (percent) and median (interquartile range), respectively. The primary endpoint was to examine the relationship between tumor volumes on anatomic MRI and 18 F-Fluciclovine PET/CT at each timepoint, and across timepoints throughout disease course. Median BTV, T1CV, and FLAIRV were compared with the Friedman test followed by post-hoc Bonferroni-adjusted pairwise comparisons at the preoperative and pre-radiation timepoints. To avoid underpowered statistical testing secondary to attrition, only BTV and T1CV were compared with the paired Wilcoxon signed rank test at the early post-radiation timepoint; these volumes were qualitatively compared without formal statistical testing at the late post-radiation timepoint. BTV-to-T1CV and FLAIR-to-BTV ratios were also reported. Additionally, changes in volume between consecutive timepoints were computed as percentages then stratified by extent of resection of the contrast-enhancing tumor [15]. An exploratory Kaplan-Meier analysis stratified by median pre-radiation residual BTV was conducted, and median OS were compared with the Breslow test. Significance level was set at 5%.

Comments (0)