
Remember me
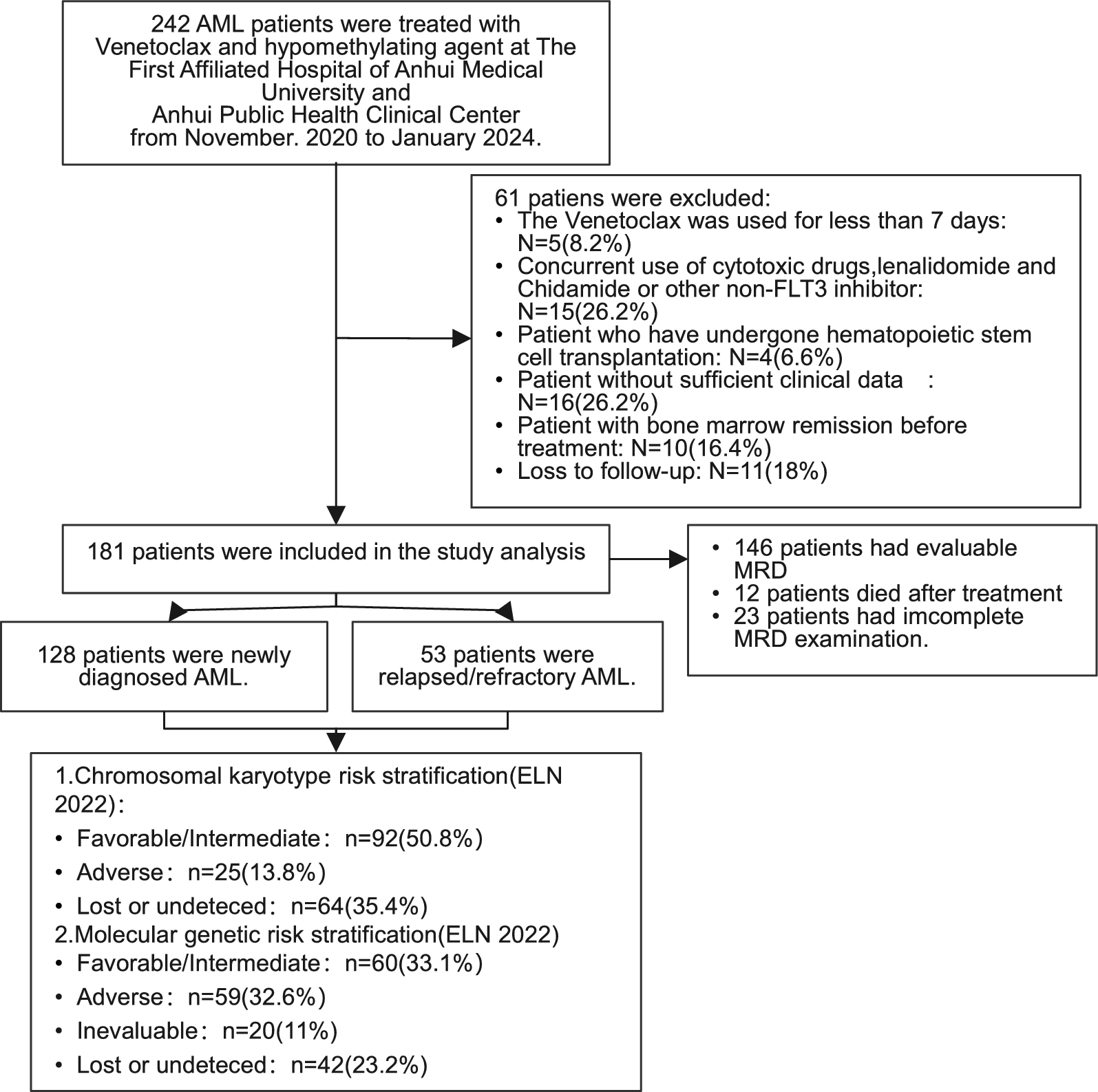
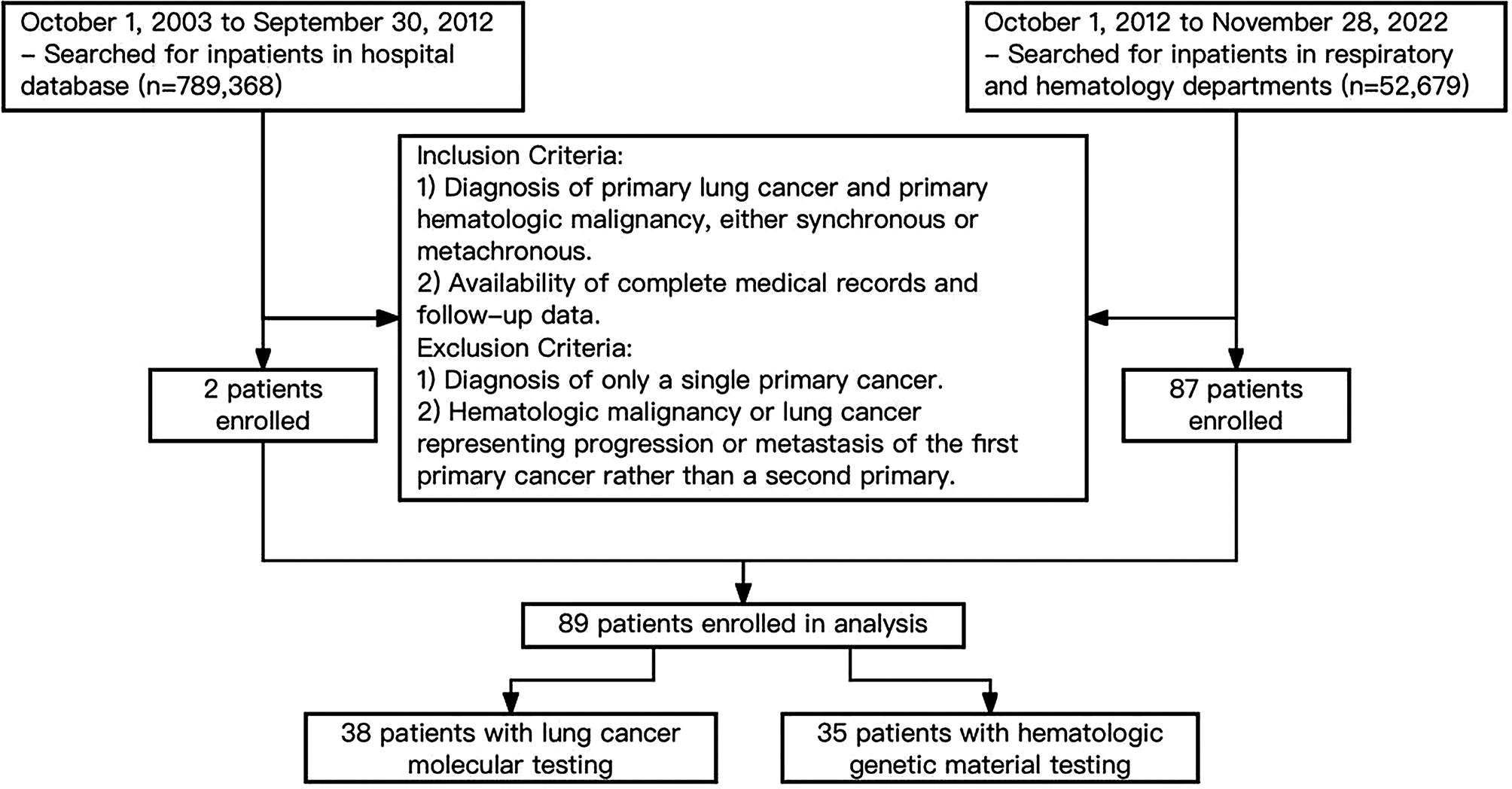

This study retrospectively included 242 patients with AML who were treated with VEN in combination with azacitidine at the First Affiliated Hospital of Anhui Medical University and the Anhui Provincial Public Health Clinical Center from October 2020 to January 2024. According to the inclusion and exclusion criteria set by this study, 61 patients were excluded due to meeting the exclusion criteria (as detailed in Fig. 1), leaving 181 patients included for further analysis. Sample size was calculated using the 10 events per predictor (EPV) principle [14], and the actual sample included in the analysis has met the statistical requirements.
Fig. 1
Flowchart of the current retrospective clinical study. AML acute myeloid leukemia, MRD minimal residual disease, ELN European Leukemia Net
The general characteristics of the 181 patients included in the study are as follows. The median age of the patients was 65 years (range: 16–90 years), with 98 males (54.1%) and 83 females (45.9%). Regarding the disease origin, 144 cases (79.6%) were classified as primary AML, while 34 cases (18.8%) had transformed from malignant hematologic diseases such as myeloproliferative neoplasms or myelodysplastic syndromes (MDS). Among these, 1 patient each had AML that had transformed from CMML-2, CML, or MPN, while the remaining 31 cases had transformed from MDS. Additionally, 3 patients (1.7%) were clinically considered to have therapy-related AML induced by toxicity following four or more cycles of chemotherapy for solid tumors. A history of exposure to HMAs was reported in 22 cases (12.2%). Among the patients, 128 were newly diagnosed with AML, while 53 had relapsed or refractory AML. Regarding treatment regimens, 166 patients (91.7%) received the VEN combined with Azacitidine regimen, while 15 patients received VEN combined with Decitabine. Additionally, 29 patients were confirmed to have FLT3-ITD mutations, among whom 12 received targeted therapy with FLT3 inhibitors such as Sorafenib or Gilteritinib.
We stratified the 181 patients according to the ELN2017, ELN2022, and LLS ELN2024 criteria. Chromosomal karyotype risk stratification according to ELN 2022 was evaluable in 117 patients, with 92 cases (78.6%) classified as low-to-intermediate risk and 25 cases (21.4%) classified as high risk. Leukemia-related gene mutation testing via the Next Generation Sequencing was completed in 139 AML patients, but molecular genetic prognosis stratification could not be accurately assessed in 20 patients due to the limited target genes covered by the testing panel. Therefore, 119 patients were eligible for molecular genetic stratification according to ELN 2022, with 60 cases (50.4%) classified as low-to-intermediate risk and 59 cases (49.6%) classified as high risk. Comprehensive stratification using ELN 2022, which includes both chromosomal karyotype and molecular genetic data, was evaluable in 111 cases, with 49 cases (44.1%) having good to intermediate prognosis and 62 cases (55.9%) having poor prognosis. Given the limited genetic information available for some patients, we also included stratification according to ELN 2017. Chromosomal karyotype risk stratification according to ELN 2017 was evaluable in 117 patients, with 89 cases (76.1%) classified as low-to-intermediate risk and 28 cases (23.9%) classified as high risk. Molecular genetic stratification according to ELN 2017 was evaluable in 125 patients, with 75 cases (60%) classified as low-to-intermediate risk and 50 cases (40%) classified as high risk. Comprehensive stratification using ELN 2017, which includes both chromosomal karyotype and molecular genetic data, was evaluable in 113 cases, with 57 cases (50.4%) having good to intermediate prognosis and 56 cases (49.6%) having poor prognosis. In 2024, the ELN updated the LLS ELN 2024 stratification, which was evaluable in 102 cases, with 49 cases (48%) having a good prognosis, 36 cases (35.3%) having an intermediate prognosis, and 17 cases (16.7%) having a poor prognosis.
The following is a map of leukemia-related gene mutations detected in all patients included in this study: 41 out of 139 cases (29.5%) had FLT3 mutations, of which 29 out of 139 cases (20.9%) had confirmed FLT3-ITD mutations; 47 out of 138 cases (34.1%) had DNMT3A mutations; 30 out of 139 cases (21.6%) had NPM1 mutations; 33 out of 137 cases (24.1%) had TET2 mutations; 31 out of 138 cases (22.5%) had CEBPA mutations, of which 16 out of 138 cases (11.6%) had confirmed CEBPA-bZIP mutations; 24 out of 137 cases (17.5%) had NRAS mutations; 19 out of 138 cases (13.8%) had IDH1 mutations; 16 out of 138 cases (11.6%) had IDH2 mutations; 17 out of 138 cases (12.3%) had TP53 mutations; 18 out of 138 cases (13%) had ASXL1 mutations; 15 out of 131 cases (11.5%) had RUNX1 mutations; 13 out of 128 cases (10.2%) had KRAS mutations; 8 out of 117 cases (6.8%) had SRSF2 mutations; 11 out of 129 cases (8.5%) had WT1 mutations; 8 out of 121 cases (6.6%) had GATA mutations; 8 out of 106 cases (7.5%) had PTPN11 mutations; 6 out of 117 cases (5.1%) had SF3B1 mutations; 7 out of 130 cases (5.4%) had BCOR mutations; and 5 out of 135 cases (3.7%) had PHF6 mutations.
Detailed clinical characteristics of the 181 patients are shown in Table 2, while the clinical characteristics of newly diagnosed AML (ND-AML) and R/R-AML are shown in Tables 3 and 4, respectively.
Efficacy evaluationAccording to the inclusion and exclusion criteria, all 181 AML patients in this study received at least 7 days of VEN + HMAs treatment. Among them, 115 patients (63.5%) achieved an overall response rate (ORR), 95 patients (52.5%) achieved complete remission (CR) or complete remission with incomplete hematologic recovery (CRi), 71 patients (39.2%) achieved CR, 20 patients (11%) achieved partial remission (PR), while 66 patients (36.5%) were non-responders (NR). Among the 181 enrolled patients in this study, 35 patients (19.3%) had missing minimal residual disease (MRD) results, including 10 patients with CR, 2 patients with PR, and 23 patients with NR. Among the 23 NR patients, 10 NR patients died during treatment. The reasons for MRD data absence in the remaining 25 patients were as follows: some were transferred to primary care hospitals for symptomatic treatment during the second evaluation; some transitioned to alternative treatment protocols (e.g., hematopoietic stem cell transplantation or bridging therapy) after completing bone marrow aspiration; and others discontinued treatment and chose to return home for palliative care. Out of 146 patients who were evaluable for minimal residual disease (MRD), 69 patients (47.3%) achieved MRD negativity, shown in Table 1.
Table 1 CR/CRi, ORR and MRD negativity rates in total, ND-AML and R/R AMLAmong the 128 ND-AML patients included in this study, 96 patients (75%) achieved ORR, 80 patients (62.5%) achieved CR/CRi, with 61 patients (47.7%) achieving CR, and 16 patients (12.5%) achieving PR, while 32 patients (25%) were NR. Out of 102 patients who were evaluable for MRD, 62 patients (60.8%) achieved MRD negativity (shown in Table 1).
Among the 53 R/R-AML patients included in this study, 19 patients (35.8%) achieved ORR, 15 patients (28.3%) achieved CR/CRi, with 10 patients (18.9%) achieving CR, and 4 patients (7.5%) achieving PR, while 34 patients (64.2%) were NR. Out of 44 patients who were evaluable for MRD, 7 patients (15.9%) achieved MRD negativity, shown in Table 1.
Factors influencing efficacy of AML patients treated with VEN combined with HMAsEvaluation of efficacy-related factors in All patientsIn the univariate analysis of factors affecting CR/CRi, this study found that mutations in the CEBPA and IDH1 genes were associated with the likelihood of achieving CR/CRi in patients treated with VEN combined with HMAs. In the univariate analysis based on MRD negativity, the study found that the type of HMAs used, age, and IDH2 gene mutations were related to the likelihood of achieving MRD negativity.
In the univariate analysis based on MRD negativity, azacitidine was associated with a better MRD negativity rate compared to decitabine (50.4% vs.15.4%; p = 0.016) (see in Table 2), and older patients appeared to achieve MRD negativity more easily than younger patients (56.1% vs. 35.9%; p = 0.015) (shown in Table 2). However, the CR/CRi rates between patients treated with azacitidine and decitabine were similar (54.2% vs. 33.3%; p = 0.121) (shown in Table 2), and there was no significant difference based on age (p = 0.309) (shown in Table 2). Additionally, several factors, including ELN2017, ELN2022, and LLS ELN2024 classifications, gender, primary AML, FAB classification, bone marrow blast percentage, ECOG score, white blood cell count, platelet count, hemoglobin levels, VEN treatment duration, and dosage, did not affect the achievement of CR/CRi or MRD negativity in patients treated with VEN combined with HMAs, shown in Table 2.
Table 2 Clinical characteristics of 181 acute myeloid leukemia patients stratified by CR/CRi and MRD negativity after induction therapy with VEN + HMAsAcross different genetic mutation subgroups, the benefit of VEN combined with HMAs was observed in all AML patients. Notably, patients with CEBPA mutations (p = 0.010) or IDH1 mutations (p = 0.046) had higher CR/CRi rates, and those with IDH2 mutations (p = 0.045) had a better MRD negativity rate (shown in Table 2). However, the presence of a CEBPA mutation or IDH1 mutation did not significantly affect the MRD negativity rate. Among the 29 patients with FLT3-ITD mutations, there was no statistical difference in CR/CRi rates between responders and non-responders, possibly due to the fact that only 12 of these patients received FLT3 inhibitors. Correspondingly, the CR/CRi rate among patients with FLT3-ITD mutations was as low as 48.3%, (shown in Table 2). In other gene subgroups, there was no significant difference in CR/CRi rates. Regardless of the treatment outcome (CR/CRi or MRD negativity), ND-AML was more likely to benefit from VEN combined with HMAs compared to R/R-AML (62.5% vs. 28.3%, p < 0.001), (shown in Table 2) suggesting that the difference might be related to the drug resistance observed in R/R-AML.
In the multivariate analysis of CR/CRi, factors with p < 0.05 were included in a logistic regression model. The results showed that R/R-AML (OR = 0.16, 95%CI 0.06–0.40, p < 0.001) was independently associated with a reduced CR/CRi rate, while the presence of CEBPA (OR = 3.70, 95%CI 1.36–10.10, p = 0.011) and IDH1 (OR = 3.60, 95%CI 1.03–12.19, p = 0.044) mutations was associated with a higher CR/CRi rate, shown in Table 2. In the multivariate analysis based on MRD, the significance of the HMAs regimen (p = 0.867), and IDH2 (p = 0.142) on MRD negativity disappeared, while age (OR = 2.38, 95%CI 1.00–5.66, p = 0.049) and R/R-AML (OR = 0.20, 95%CI 0.06–0.63 p = 0.006) remained an independent influencing factor for MRD negativity, shown in Table 2.
Evaluation of efficacy-related factors in newly diagnosed and R/R-AML patients, respectivelyIn the univariate analysis of ND-AML, primary AML showed a better CR/CRi rate compared to secondary AML (67% vs. 44%, p = 0.033) (shown in Table 3). Furthermore, in the ELN2017 and ELN2022 cytogenetic risk subgroups, AML patients in the favorable and intermediate risk groups responded better to VEN combined with HMAs therapy than those in the adverse risk group (p < 0.05) (shown in Table 3). In the gene mutation subgroup analysis, CEBPA mutations (p = 0.049) were associated with a higher remission rate, shown in Table 3. However, in the multivariate analysis, the significance of primary AML, favorable or intermediate cytogenetic risk, and CEBPA mutations on the CR/CRi rate disappeared. Regarding MRD negativity, there was no significant difference based on primary AML, cytogenetic risk stratification, or the presence of CEBPA mutations. Additionally, no significant impact on treatment response in ND-AML was observed across different subgroups based on baseline characteristics and disease features, including age, gender, FAB classification, ECOG score, white blood cell count, platelet count, hemoglobin levels, bone marrow blast percentage, HMAs regimen, VEN treatment duration and dosage, ELN2017 risk stratification, molecular genetic stratification, ELN2022 risk stratification, and LLS ELN2024 precision risk stratification (shown in Table 3).
Table 3 Clinical characteristics of 128 newly diagnosed acute myeloid leukemia patients stratified by CR/Cri and MRD negativity after induction therapy with VEN + HMAsIn the univariate analysis of CR/CRi in R/R-AML, we observed that DNMT3A mutations were associated with a poorer CR/CRi rate (none of the 10 patients with the mutation achieved CR/CRi) (shown in Table 4). Although there was no statistical difference in the CR/CRi rate between IDH1 mutant and non-mutant patients, the response rate among IDH1 mutant patients reached 75%, indicating a trend toward better prognosis. Additionally, in the univariate analysis based on MRD, IDH1 mutations were associated with a better MRD negativity rate, shown in Supplementary Table 1. There were no statistically significant differences observed in the effects of age, gender, FAB classification, ECOG score, white blood cell count, platelet count, hemoglobin levels, bone marrow blast percentage, HMAs regimen, cytogenetic stratification, ELN2017 risk stratification, molecular genetic stratification, ELN2022 risk stratification, LLS ELN2024 risk stratification, VEN treatment duration, VEN dosage, and different genetic mutation subgroups on the efficacy of VEN combined with HMAs therapy for at least 7 days (shown in Table 4).
Table 4 Clinical characteristics of 53 relapsed/refractory acute myeloid leukemia patients stratified by CR/CRi and MRD negativity after induction therapy with VEN + HMAsComparison of efficacy-related factors between ND-AML and R/R-AML patients receiving VEN combined with HMAsUnivariate analysis based on CR/CRi and MRD showed that ND-AML had a better treatment response compared to R/R-AML. Therefore, further subgroup analysis was conducted for ND-AML and R/R-AML. The results demonstrated that across various subgroups, including age, gender, FAB classification, ECOG score, and bone marrow blast cell percentage stratifications, ND-AML patients benefited more from VEN combined with HMAs, achieving higher remission rates than R/R-AML patients (shown in Fig. 2).
Fig. 2
Subgroup Analysis Comparing the Efficacy of VEN + HMAs Induction Therapy in ND- and R/R-AML Patients Stratified by CR/CRi. ND newly diagnosed, R/R relapsed/refractory, OR odds ratio, CI confidence interval, HMA hypomethylating agent, ELN European Leukemia Net, FAB French-American-British classification systems, ECOG Eastern Cooperative Oncology Group
In the primary AML subgroup, ND-AML had a higher remission rate. However, in the secondary AML subgroup, the CR/CRi rates between ND-AML and R/R-AML were similar, suggesting that secondary AML might be a factor leading to poor prognosis. Regarding the choice of HMAs, ND-AML showed better treatment outcomes with azacitidine compared to R/R-AML (OR = 0.25, 95% CI 0.12–0.54, p < 0.001) (shown in Fig. 2). However, there was no significant difference in benefit between the two groups with decitabine (OR = 0.17, 95% CI 0.01–2.56, p = 0.199), shown in Fig. 2.
Different VEN dosage gradients, 100 mg, 200 mg, and 400 mg, showed significant differences in remission rates in both ND-AML and R/R-AML groups (p < 0.05), shown in Supplementary Fig. 2. However, there was no significant difference in CR/CRi between ND-AML and R/R-AML patients with low VEN blood concentrations or those who took VEN for less than 21 days. In contrast, when higher VEN blood concentrations were achieved (OR = 0.11, 95% CI 0.02–0.45, p = 0.002) or when VEN was taken for more than 21 days (p < 0.05), shown in Fig. 2. ND-AML had a better remission rate than R/R-AML. This suggests that extending the duration of VEN treatment and optimizing its blood concentration levels could potentially enhance therapeutic outcomes for patients.
There was no significant difference in CR/CRi rates between ND-AML and R/R-AML in the poor prognosis subgroups of ELN2017 and its cytogenetic risk stratification and molecular genetics stratification, as well as ELN2022 risk stratification and its cytogenetic risk stratification and molecular genetics stratification (shown in Fig. 2). However, significant differences were observed in the favorable or intermediate prognosis groups, with ND-AML showing better remission rates compared to the poor prognosis group. In the gene mutation subgroup analysis of ND-AML and R/R-AML, significant differences in remission rates were observed in patients with FLT3 and TET2 mutations, with ND-AML showing better remission rates. However, no significant differences in remission rates were observed in other gene mutation subgroups, including TP53, NPM1, and IDH2 mutations (shown in Fig. 2).
Comparison of efficacy between different VEN treatment durationsAmong 181 patients, those who received VEN for 7–14 days (n = 26, 55.3%), 14–21 days (n = 18, 54.5%), and 21–28 days (n = 51, 50.5%) had similar CR/CRi rates (p = 0.832) (shown in Table 5). No significant differences were observed in the corresponding MRD-negative rates either (57.1% vs.46.2% vs.43.5%, p = 0.395) [shown in Table 5 (A1&A2)].
A similar pattern was observed in both ND-AML and R/R-AML. For ND-AML patients, those treated with VEN for 7–14 days (n = 20, 62.5%), 14–21 days (n = 14, 63.6%), and 21–28 days (n = 46, 62.2%; p = 0.992) also had no significant difference in CR/CRi rates. The corresponding MRD-negative rates were 70.8%, 58.8% and 57.4%, respectively (p = 0.511) [shown in Table 5 (B1&B2)]. In R/R-AML patients, those treated with VEN for 7–14 days (n = 6, 40%), 14–21 days (n = 4, 36.4%), and 21–28 days (n = 5, 18.5%; p = 0.268) had similar CR/CRi rates as well, with no significant differences in corresponding MRD-negative rates (27.3%, 22.2% and 8.3% respectively; p = 0.305) [shown in Table 5 (C1&C2)].
In a separate analysis of the 181 patients according to ELN 2022 prognosis, including those with adverse prognosis (n = 62) and non-adverse prognosis (n = 49), the CR/CRi rates were similar between adverse and non-adverse prognosis groups within each VEN treatment duration: 7–14 days (adverse vs. non-adverse, n = 8, 66.7% vs. n = 9, 47.4%), 14–21 days (n = 7, 58.3% vs. n = 7, 77.8%), and 21–28 days (n = 21, 55.3% vs. n = 15, 71.4%) (adverse vs. non-adverse, p = 0.784 vs. p = 0.175). No significant differences were observed in the corresponding MRD-negative rates either (adverse vs. non-adverse, p = 0.692 vs. p = 0.993) [shown in Table 5 (A1&A2)].
Similarly, in the LLS ELN 2024 precision risk stratification, there were no significant differences in CR/CRi rates across low-risk (n = 49), intermediate-risk (n = 36), and high-risk (n = 17) groups among patients receiving VEN for 7–14 days (low vs. intermediate vs. high, 47.4% vs. 57.1% vs. 75%), 14–21 days (77.8% vs. 62.5% vs. 33.3%), and 21–28 days (71.4% vs. 61.9% vs. 80%) (p = 0.175 vs. p = 1.000 vs. p = 0.282). No significant differences were found in the corresponding MRD-negative rates either (p = 0.473 vs. p = 0.785 vs. p = 0.993) [shown in Table 5 (A1&A2)]. Similar results were observed in both ND-AML and R/R-AML, as shown in Table 5 (B&C).
The duration of VEN treatment did not appear to affect CR/CRi rates in patients with CEBPA mutations (n = 31) or IDH1 mutations (n = 19). There were no significant differences in CR/CRi rates among those treated with VEN for 7–14 days (n = 6, 66.7% vs. n = 5, 83.3%), 14–21 days (n = 4, 80% vs. n = 4, 100%), and 21–28 days (n = 14, 82.4% vs. n = 6, 66.7%) (p = 0.837 vs. p = 0.498). Similarly, the MRD-negative rates were also comparable (p = 1.000 vs. p = 1.000) (shown in Table 5 (A1&A2).
Relationship between VEN treatment duration and hematologic adverse eventsFollowing VEN combined with a HMAs regimen, 174 patients experienced grade ≥ 3 hematologic adverse events, with 5 patients lost to follow-up after discharge. Neutropenia was the most common adverse event, occurring in 176 patients (97%), with 169 cases (96%) being grade ≥ 3. Anemia was the second most common, also occurring in 176 patients (97%), with 163 cases (92.6%) being grade ≥ 3. Thrombocytopenia was observed in 175 patients (96.7%), with 155 cases (88.6%) being grade ≥ 3 thrombocytopenia.
Due to the impact of the disease, many patients already exhibited hematologic abnormalities before starting the treatment. Therefore, the safety analysis included only 40 patients who met the baseline criteria of absolute neutrophil count (ANC) ≥ 0.5*109/L, hemoglobin ≥ 60 g/L, and platelet count ≥ 20*109/L, and who achieved ORR. Among these patients, no significant differences were found in the incidence of ANC < 0.5*109/L, platelet count < 20*109/L, or hemoglobin < 60 g/L between those treated with VEN for 7–14 days, 14–21 days, and 21–28 days. Even after adjusting for the impact of age, no differences in the incidence of hematologic adverse events were observed between the different durations of VEN treatment. Similarly, the time to transfusion independence for all three blood lineages was approximately the same for patients treated with VEN for 7–14 days, 14–21 days, and 21–28 days. A separate analysis of ND-AML showed similar results [shown in Table 5 (D1&D2)].
Comments (0)