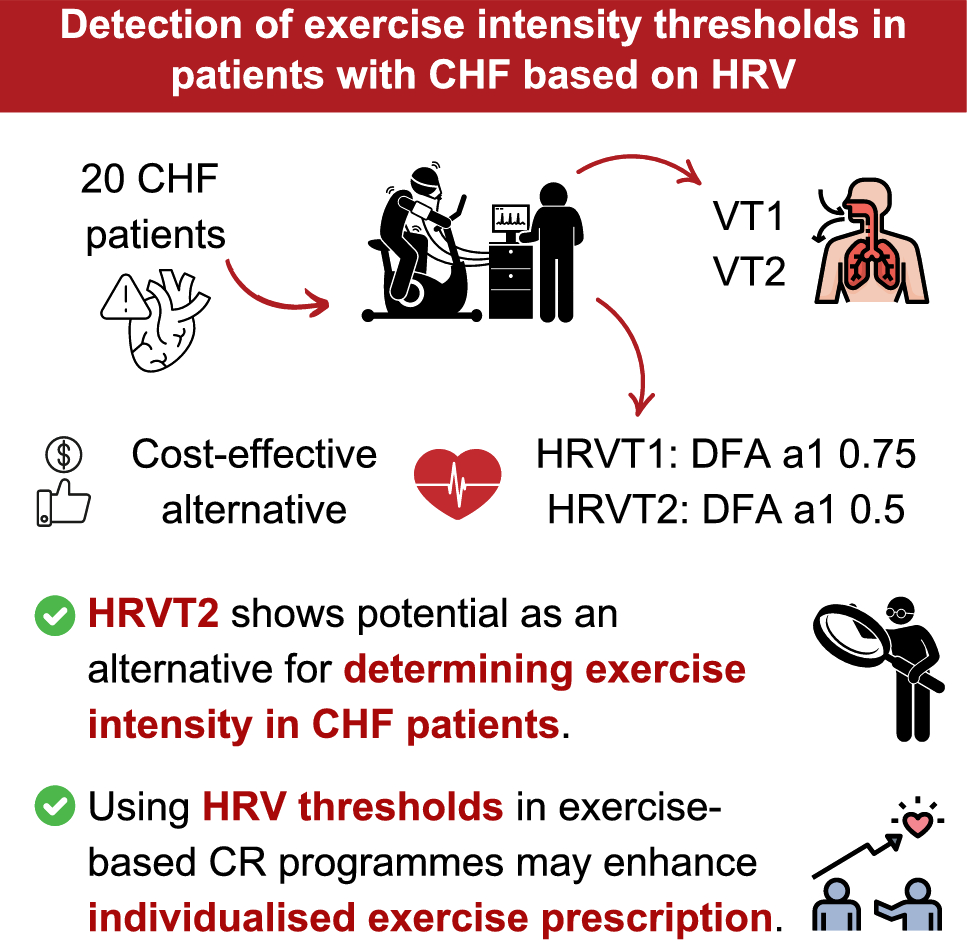
The aim of this study was to assess the level of agreement between ventilatory and HRV thresholds in patients with CHF. Our initial hypothesis suggested a strong agreement between VT1 and HRVT1, based on a previous study conducted with cardiac patients, most of them with coronary artery disease (Rogers et al. 2021d) and that HRVT2 would show at least moderate concordance with VT2. The findings partly confirmed this hypothesis: HRVT2 displayed strong agreement with VT2 across all outcome variables, whereas HRVT1 achieved only low to moderate correlations with VT1.
Agreement between HRVT1 and VT1
Regarding the first threshold, correlations between HRVT1 and VT1 varied across the measured variables. A non-significant, low correlation was observed for HR, while PO and VO2 showed significant low and moderate correlations, respectively. Despite these associations, the limits of agreement were wide for all variables. These findings contrast with those of Rogers et al. (2021d), who reported significant and strong correlations (r = 0.86 in HR, r = 0.87 in PO, r = 0.95 in VO2) with lower mean biases (3 ± 7 bpm, 5 ± 13 W, and 1.2 ± 2.9 ml·kg−1·min−1). Nevertheless, they presented wider limits of agreement (− 11 to 18 bpm, − 20 to 31 W, and − 4.6 to 7 ml·kg−1·min−1). Despite these differences, both studies consistently found that HRVT1 values were higher than VT1 values. While the limits of agreement between HRVT1 and VT1 remained wide, they are comparable to the ranges observed in studies comparing ventilatory and lactate thresholds (Pallarés et al. 2016) suggesting that such variability is consistent with standard threshold identification methods. Such disparities could stem from methodological differences, particularly in the determination of VT1. For instance, Rogers et al. (2021d) utilised the excess CO2 method with unaveraged breath-by-breath data, whereas we adopted a mixed method using averaged ventilatory data. Moreover, differences in patient populations could also contribute to these discrepancies. In the cited study, most participants had coronary artery disease, a condition that generally represents a less advanced stage of cardiovascular dysfunction compared to CHF, what may have influenced the results.
Additionally, differences in ECG recording devices might have influenced results. Rogers et al. (2021d) used a device with a lower sampling rate of 200 Hz, while our study employed an 8000 Hz sampling rate. Previous research has shown significant variations in DFA a1 values at rest when comparing devices with different sampling rates. Specifically, lower sampling frequencies introduce greater errors in RR interval detection, which can affect HRV measurements, particularly when HRV values are low (Tapanainen et al. 1999).
The use of beta-blockers by patients in this study may have further influenced the relationship between HRVT1 and VT1. Beta-blockers primarily block beta-adrenergic receptors, thereby limiting heart’s response to increases in circulating catecholamines without necessarily reducing sympathetic outflow (Hori et al. 1991). Because DFA a1 thresholds depend on the dynamic interaction between sympathetic and parasympathetic branches, this pharmacological modulation may have resulted in a blunted chronotropic response, potentially affecting the accuracy of HRVT1 estimations. Although parasympathetic withdrawal remains a key factor influencing HRV during exercise, the attenuated decline in HRV caused by partial beta-adrenergic blockade could still lead to a weaker correlation with VT1 (Ishida et al. 1997). In a recent randomized, placebo-controlled trial, acute cardioselective beta1-blockade (bisoprolol) in healthy adults had no significant impact on ventilatory efficiency or the ventilatory threshold, suggesting that the effect may be limited or population-specific (Forton et al. 2022). In this study, tests were scheduled in the afternoon to minimise acute effects from morning doses; nevertheless, residual activity due to variable half-lives and individual responses may persist. Finally, differences in the testing times across studies, such as in Rogers et al. (2021d), could contribute to variability in reported correlations.
Agreement between HRVT2 and VT2
In contrast to HRVT1, HRVT2 showed stronger agreement with VT2. To the best of our knowledge, this is the first study to evaluate HRVT2 in cardiac population, specifically in patients with CHF. Our results indicate strong correlations between both methods, with the strongest agreement observed in VO2 and HR values. These results align with prior studies that evaluated this threshold in healthy populations. For example, Rogers et al. (2021c) reported similar findings in recreational male runners during an incremental treadmill test in HR values determined by the two methods (r = 0.78; mean bias − 4 ± 10 bpm, limits of agreement from − 24 to 16 bpm). Likewise, Schaffarczyk et al. (2022) reported even stronger correlation in a female cohort (Pearson’s r = 0.90; mean bias 0.5 ± 5.7 bpm). Additionally, Sempere-Ruiz et al. (2024) found similar results when examining HRVT2 in a population of healthy participants, reporting correlations exceeding r = 0.80 and narrower limits of agreement compared to HRVT1. These findings further reinforce the potential utility of the DFA a1 method as a reliable approach for determining the second threshold in patients with CHF. This is particularly relevant for exercise prescription in this population, as high-intensity aerobic training (above the second threshold) has been shown to be highly effective in CHF patients, improving cardiorespiratory fitness, vascular function, and overall prognosis (Turri-Silva et al. 2021; Fuertes-Kenneally et al. 2023).
Mechanistically, the correlation between DFA a1 and ventilatory thresholds may be explained by their shared reflection of systemic physiological responses to exercise. This stage marks a progressive transition in the relative contribution of metabolic pathways, with a gradual increase in anaerobic glycolysis as exercise intensity rises, which are accompanied by changes in ANS activity. DFA a1, as a non-linear HRV metric, is sensitive to alterations in ANS regulation, particularly the balance between sympathetic and parasympathetic inputs. Rogers et al. (2021c) proposed that the progressive loss of fractal-like properties in HRV, reflected in decreases in DFA a1, corresponds to increased physiological stress and the body's struggle to maintain homeostasis at higher exercise intensities. This conceptual overlap suggests that DFA a1 can serve as a surrogate marker for ventilatory thresholds, providing a cost-effective and accessible method for exercise intensity prescription.
Clinical applications
HRVT2 showed good agreement with VT2, supporting its potential as a practical surrogate for defining the upper boundary of the heavy-intensity domain in cardiac-rehabilitation settings where CPET is unavailable, enhancing the precision of exercise prescription. This perspective aligns with the concerns highlighted by Keir (2024) regarding the challenges and limitations of CPET in clinical practice, such as cost, accessibility, and patient burden. In contrast, HRVT1 displayed only modest correspondence with VT1. Until larger CHF cohorts confirm its validity, HRVT1 should be used with caution and preferably in combination with other sub-maximal markers.
Nonetheless, the operational simplicity of DFA a1 calculation—single-channel RR recording from a HR monitor or ECG, and fixed cutoff values for HRVT1 (0.75) and HRVT2 (0.5) that are presumed to remain stable regardless day-to-day training and fatigue—remains attractive. Clinicians could employ HRVT2 to individualise interval workloads, to verify whether a bout remained below or above the second threshold, or to adjust home-based programmes without previous laboratory gas analysis, providing a promising framework for real-time monitoring and individualised adjustment of training intensity.
Study limitations and future research
Several limitations must be acknowledged. First, because no a priori sample-size estimation was performed, we cannot ascertain whether the study was adequately powered to detect smaller between-method differences. However, differences between the two methods were estimated as a measure of effect size magnitude. Second, a high number of patients were excluded from the analysis due to difficulties in detecting first and second thresholds. This challenge is common in studies employing CPET in clinical populations. Keir (2024) highlighted that the identification of ventilatory thresholds in patients with cardiac pathologies is often compromised by individual physiological variability, methodological inconsistencies, and technical limitations. Furthermore, these factors may be exacerbated in CHF patients, where disease-related alterations in ventilatory and cardiovascular responses further complicate the accurate determination of thresholds. Consequently, the observed data loss in our study aligns with previously reported challenges in applying CPET-derived thresholds in clinical settings, reinforcing the need for alternative, more accessible methods for exercise intensity prescription. Third, our sample was predominantly male (65%), and the small number of women (n = 7) precluded a statistically powered sex-stratified analysis. Future studies with larger and more balanced cohorts are required to determine whether the present findings generalise equally to males and females. Finally, all participants were stable NYHA class II–III heart-failure patients treated according to contemporary guidelines; caution is warranted when extrapolating the results to other heart-failure phenotypes or to patients with more advanced functional limitation.
Future research should aim to validate these findings in larger, more diverse cohorts and explore the longitudinal applicability of HRV thresholds in CHF management. Additionally, it should focus on validating the use of DFA a1 across a broader range of populations and pathologies, including individuals with other chronic conditions such as chronic obstructive pulmonary disease or metabolic syndrome. Additionally, further investigation is needed to confirm the reliability of DFA a1 in delineating exercise intensity domains during prolonged and repeated sessions. This includes exploring how factors like fatigue and long-term training adaptations might influence exercise intensity thresholds. Combining DFA a1 with complementary methods, such as near-infrared spectroscopy, could also enhance the precision of exercise monitoring by providing a more comprehensive view of systemic and local muscle oxygenation responses. Ultimately, these efforts will help establish DFA a1 as a versatile and widely applicable tool for exercise prescription and monitoring.

Comments (0)