In this study, we have investigated associations between markers of inflammatory status and adiposity and bone phenotype in men and women. Overall, these data suggest modest associations between some markers of inflammatory status and adiposity, which together with an increasing number of risk factors, may influence healthy bone ageing. The use of both pQCT and DXA data helps to elucidate these relationships beyond those with DXA aBMD and, therefore, contributes to our understanding of the specific relationships with different aspects of bone phenotype. Higher adiponectin was also associated with the odds of having a fragility fracture during adulthood in women; however, this association did not reach statistical significance.
Higher IL-6 levels were associated with higher aBMD at the spine and whole body in women; in men, higher IL-6 levels were associated with lower trabecular and total vBMD. In the Hertfordshire Cohort Study, there were no associations between IL-6 and lumbar spine or femoral neck aBMD in cross-sectional analyses; these results were adjusted for gender and are consistent with the results which we found in men in NSHD [32]. Similarly, results from the Framingham Osteoporosis Study, showing a lack of associations between IL-6 and aBMD at the hip and spine, are also in agreement with our findings. The relationships which we found between higher IL-6 and higher aBMD at the spine and whole body in women are not consistent with results in the literature which report a negative, or lack of, association between IL-6 and aBMD [33, 34]. Interestingly, in the Framingham Osteoporosis Study, a relationship between CRP (an acute phase inflammatory marker downstream of IL-6) and higher femoral neck aBMD was observed in postmenopausal women using menopausal hormone therapy [35]. It is possible that the associations were due to another non-mechanical factor in the relationship between fat mass and bone or differences in age between studies. One of the strengths of NSHD is that all participants are born within a week of one another, limiting confounding by age.
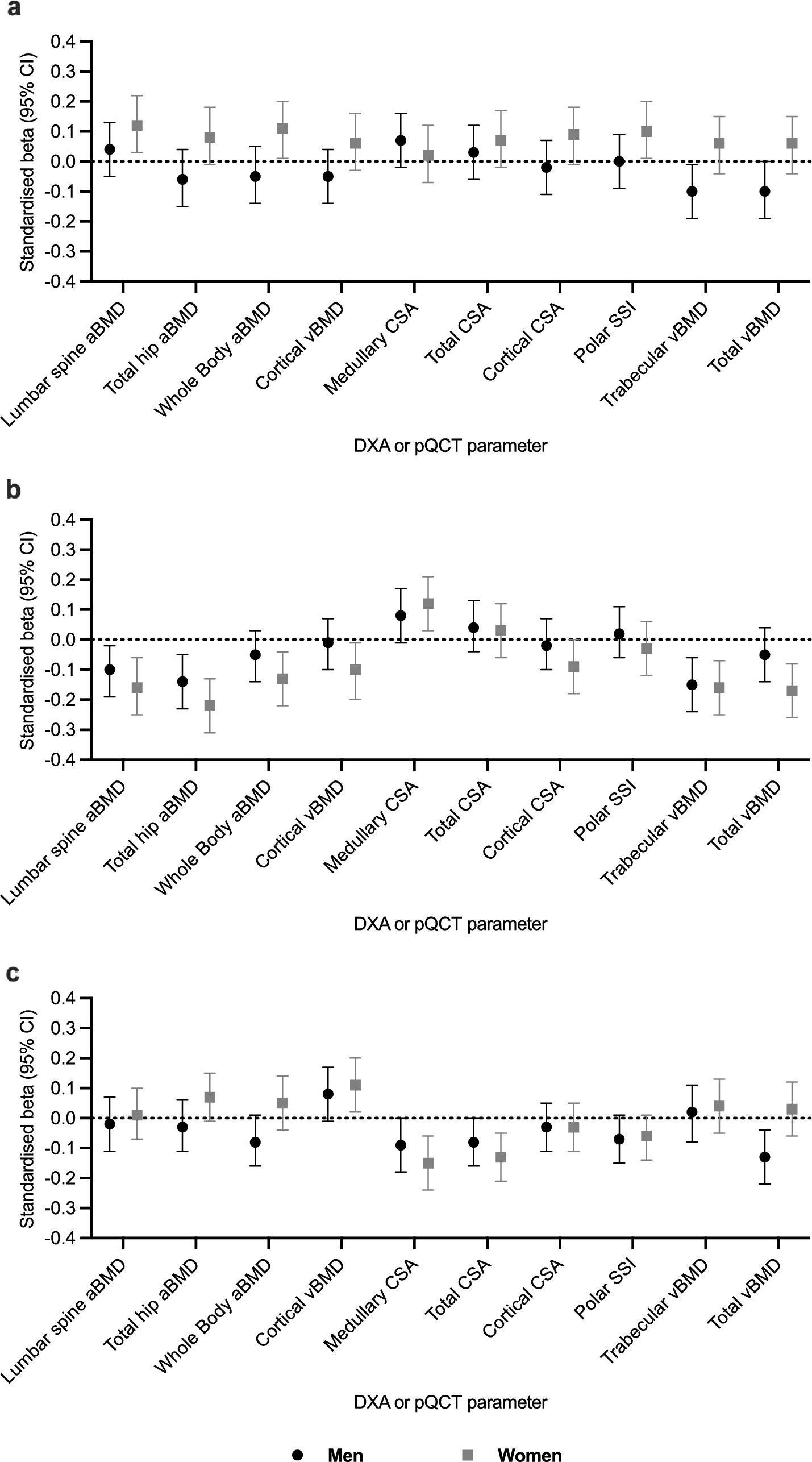
We observed that higher adiponectin was related to lower aBMD in men and women which is consistent with findings from the Hertfordshire Cohort Study: at the lumbar spine, an SD increase in adiponectin was associated with 0.11 [− 0.21, − 0.01] lower aBMD in fully adjusted models, which included adjustment for gender, age, height, weight adjusted for height residuals, smoking, alcohol, diet, physical activity and hormone replacement therapy [32]. After full adjustment, we observed a similar effect size at the spine in men (− 0.10 SD [− 0.19, − 0.02]) and women (− 0.16 SD [− 0.25, − 0.06]). Associations between adiponectin and pQCT-measured vBMD were also previously reported in the InChianti study [20]. Similar to our results, relationships were observed between adiponectin and cortical, trabecular and total vBMD in women; however, in contrast, there were no associations in men, and there was a significant interaction between gender and adiponectin in the relationship with cortical and trabecular vBMD. Finally, in another study in postmenopausal women (mean age: 62.3 years), adiponectin was negatively associated with total vBMD of the distal tibia [24]. This is consistent with the relationship we observed between adiponectin and total vBMD at the 4% radius in women in NSHD.
The direction of association between leptin and aBMD is consistent with results from the Rancho Bernardo study, in which higher leptin was related to higher aBMD in women only [15]. In addition, in the Rancho Bernardo study there was also an association at the lumbar spine. In the Hertfordshire Cohort Study, there were positive associations between leptin and femoral neck aBMD with adjustment for gender, but these were attenuated after adjustment for lifestyle factors [32]. In our study, a relationship between higher leptin levels and lower total vBMD was observed in men. Similar to our study, in young men (mean age: 18.9 years) there were also no associations between leptin and cortical vBMD or trabecular vBMD of the radius in fully adjusted models; however, in contrast to our results this study reported a negative association between leptin and cortical CSA [23]. In postmenopausal women, leptin concentration was negatively associated with total CSA of the tibia diaphysis [24]. Consistent with this, in our study, we found a relationship between higher leptin levels and lower total CSA at the 50% radius, which may help to demonstrate the contrasting direct and indirect effects of leptin on bone.
During our study, we found small effect sizes in the relationships between IL-6, leptin, and adiponectin, and bone phenotype. Clinically, DXA-measured BMD is a known predictor of fracture risk and, at age 65, per SD decrease in hip BMD, the risk of osteoporotic fracture increases by 1.41 (risk ratio: 1.41 [95% CI 1.33–1.51]) in men and by 1.38 in women (risk ratio: 1.38 [95% CI 1.28–1.48]) [36].
Associations of the markers of inflammatory status and adiposity with DXA and pQCT parameters did not translate into associations with prevalent fragility fractures. Similarly, in the Cardiovascular Health Study there was no association between IL-6 and a composite of incident fractures (including hip, pelvis, humerus or proximal forearm) in men and women [10]. In the Health ABC study, inflammatory markers were associated with an increased risk of fracture; however, the association between IL-6 and incident fracture risk was not statistically significant after adjustment for confounders [11]. In contrast to our results, in the Study of Osteoporotic Fractures, women in the highest IL-6 quartile had a greater risk of fracture compared to women in the lower IL-6 quartiles [9]. For adiponectin, negative associations with BMD, but not with fracture risk, have been shown [37]. Interestingly, in the Health ABC study, higher adiponectin levels in men, but not women, were associated with an increased risk of fracture after adjustment for confounders; however, consistent with our results, leptin was not associated with fracture risk in men or women [21]. Sex differences in the association between adiponectin and vertebral fractures were reported in the Rancho Bernardo Study, with higher adiponectin levels associated with an increased risk of vertebral fractures in men but not women [38]. Previously published results concerning the relationship between these markers of adiposity and inflammation with fracture are therefore conflicting. It is also possible that some of the differences between these studies could be due to differences in the type of fracture, such as traumatic or non-traumatic, or fracture sites, included in the studies.
In addition to clinical studies, preclinical studies have shown direct links between IL-6, adiponectin, and leptin and bone metabolism. IL-6 is known to induce osteoclast formation in vitro [39]. In addition, there are also links between IL-6 and osteoblasts, and IL-6 knockout mice showed enhanced bone formation following stress fractures [40]. Adiponectin has been shown to inhibit osteoclast formation in vitro [41] and adiponectin-deficient mice were shown to have reduced bone mass [42]. It is known that the action of leptin on bone varies depending on its direct and indirect action, which accounts for the fact that contrasting effects have been observed [13]. In vitro, leptin has been shown to inhibit osteoclast generation [43] and leptin-deficient mice were shown to have decreased bone growth and lower osteoblast-lined bone perimeter, both of which increased when leptin was administered [44].
Hormonal mechanisms may explain the differences in relationships between markers of inflammation and bone between men and women. For example, it is well-established that estrogen plays a major role in bone metabolism and, as an inhibitor of bone resorption, the loss of estrogen helps to explain bone loss in postmenopausal women [45]. It is also possible that additional aspects of body composition contribute to differences in bone health between men and women. In addition to body composition, there are also changes in measures of muscle strength and function, such as grip strength, with age in later life, the change in which shows correlations with hip BMD [46]. Of note, android to gynoid fat mass ratio, a marker of adipose distribution, has been shown to have negative associations with DXA-measured BMD in women but not men [47].
Indeed, it has been suggested that the relationship between fat and bone mass shows differences between men and women [48]. This is in agreement with the differences in the relationships which we found and, in addition, we found higher adiponectin levels in women compared to men. In addition, it has been shown that different adipose tissue deposits have different relationships with markers of adiposity, for example, visceral adipose tissue has a greater association with adiponectin, while subcutaneous adipose tissue has a greater association with leptin [49]. These differences may play an important role in the differences in the relationship between adiposity, inflammation, and bone.
A limitation of this study was that our sample did not include all NSHD participants who were assessed at age 60–64 years (maximum population size at 60–64 years: men: 1067, women: 1161; analysis sample size: men: 498, women: 474) and this limited our statistical power, and likely introduced bias, to detect associations. A further limitation is that fragility fractures were defined based on self-report of a broken bone (at an osteoporotic site or by a low-trauma mechanism) since 25 years of age, and it is therefore possible that there could be recall bias. Although we adjusted for smoking status, physical activity, social class, and ever-use of HRT in women, it is also possible that additional confounders, such as medication use and diet, may also have had the potential to influence the results we observed. Regarding diet, calcium and vitamin D and protein intake are important aspects of diet, which are known to be related to bone health [1, 29]. In addition, following a Mediterranean diet, or a nutrient-rich diet, both of which include nutrients with anti-inflammatory action, is likely to have a protective effect on bone via the reduction of oxidative stress [29, 50]. It may also be possible that other medications, which act via inflammatory pathways, played a role in the relationships between inflammation and bone. Finally, it has been shown that different types of exercise have different effects on BMD [51]. It is therefore possible that the type of exercise which participants undertook, such as weight bearing or non-weight bearing, resistance exercise, played a role in these relationships.
Finally, with subjects having all been born in the same week of the same year, the results may not be generalisable to other cohorts, especially as the NSHD cohort was born in the early post-war period, with specific conditions which may not have been seen in later cohorts. However, it is also a strength of our study that all participants were born in the same week in March 1946, as there is confidence that the associations are not confounded by age.
The use of fracture data, in addition to clinical measurements, is also a strength of our study. A further strength was the use of fat mass residuals, which enabled adjustment for body composition without introducing multi-colinearity between highly correlated predictors. We also used a novel method, the calculation of leptin residuals, which enabled the effect of leptin which remains after adjustment for fat mass to be investigated. A final strength is that participants had both DXA and pQCT measures of bone phenotype. This enabled the comparison of DXA with pQCT, which is independent of body size and able to measure the density of the trabecular and cortical compartments separately. Our results showed that, in some instances, while there was no association between a marker and DXA aBMD, there were associations with pQCT parameters.

Comments (0)