There are very few reports of non-orthopedic surgery having been undertaken in people with severe osteogenesis imperfecta. A literature search identified only three instances, all of which were done laparoscopically; one for a ruptured appendix [5], another for a tubo-ovarian abscess [6], and a third for bariatric surgery [7]. Guidelines for orthopaedic surgery in OI emphasise that decisions around any surgical procedure should involve the patient and family, coupled with a multidisciplinary team [8, 9]. The challenges of anaesthetic management of individuals with severe OI undergoing orthopaedic surgery have also been published [10, 11].
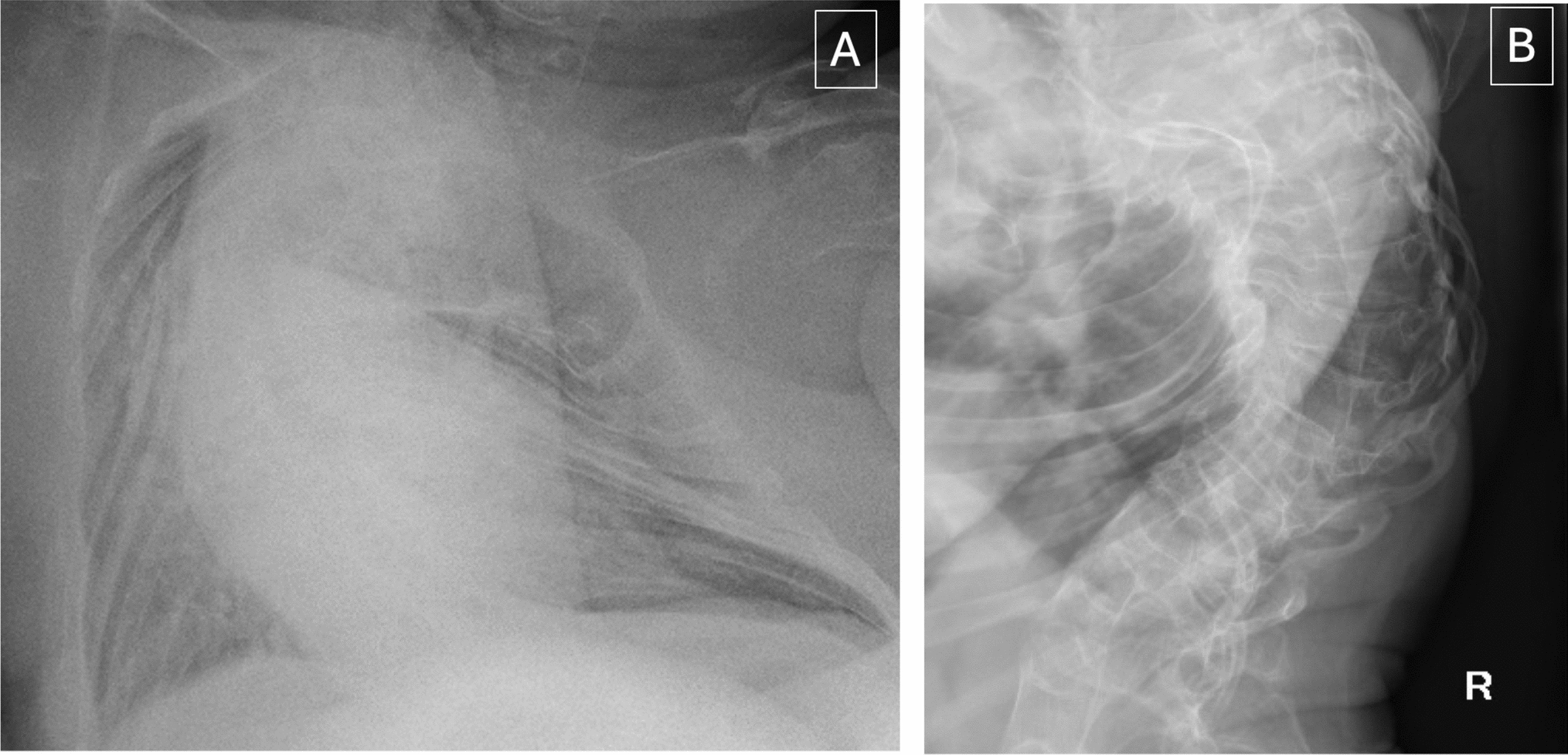
In this case, there was extensive discussion with co-author JA (the patient) and all members of the care team before the surgery in view of the potential risks involved. The decision was made to go ahead with surgery as that the patient’s quality of life was severely impaired as the result of the recurrent episodes of abdominal pain and it was felt that on balance, the benefits outweighed the risk. Many of the anaesthetic considerations when managing a patient with OI will be pertinent irrespective of the patient’s age or the type of surgery being conducted. There is potential for difficult airway management, risk of fractures when positioning (including cervical spine injury during airway manipulation), and with the use of suxamethonium and non-invasive blood pressure cuffs [12]. Sites for intravenous access may be limited due to fractures and musculoskeletal deformity. The risk of hypermetabolic hyperthermia and sensitivity to neuromuscular blocking drugs has been reported to be increased in OI although this is mainly based on case reports [13] and one case series of 49 OI patients undergoing surgery found no evidence to suggest that the risk of hypermetabolic hyperthermia was increased [14]. In this case, there was no evidence of hyperthermia.
Traditional teaching also advises avoiding suxamethonium in OI because of concerns regarding an acute hyperkalaemic response and contraction-induced fractures [15]. These complications have been reported in patients with various neuromuscular diseases and immobilisation [16]. This was the reason that we used rocuronium as a muscle relaxant. Although the patient had had residual neuromuscular blockade several hours postoperatively, this was successfully reversed with sugammadex.
The patient was treated with laparoscopic surgery. This now represents the standard approach for cholecystectomy in the UK, offering a number of advantages over open surgery, including reduced post-operative pain and enhanced recovery. The main anaesthetic concern in laparoscopic surgery is the presence of pneumoperitoneum and its impact on the cardio-respiratory and musculoskeletal systems; this additionally complicates the management of anaesthesia in a patient with OI. The raised intra-abdominal pressure associated with pneumoperitoneum inhibits effective ventilation by increasing pressure under the diaphragm and simultaneously increasing intra-thoracic pressure; this could result in lung barotrauma, rib fractures and development of pneumothoraxes. Ventilation is also impaired by systemic absorption of carbon dioxide, the gas used for insufflation of the abdominal cavity. An intra-abdominal pressure of 12 mmHg was achieved cautiously and allowed adequate surgical access with carbon dioxide controlled at near normal levels for this patient. Ventilation probably benefitted from the reverse Trendelenburg position used in this case. Intercostal chest drain insertion was discussed and prepared for but was not required.
There was a chance that the laparoscopic approach described would not be possible in this case due to the patient’s body habitus, inability to lie flat, and the extremely short distance between xiphisternum and umbilicus, all of which would restrict access to the peritoneum. Pre-operative multidisciplinary discussion focussed heavily on this as well as the risks associated with open surgery. Conversion to open cholecystectomy was not felt to be in the patient’s best interests due to the increased risks of a larger incision; rib retraction; difficult to manage post-operative pain; and likelihood of prolonged ventilation and critical care stay. The patient was in complete agreement with the multidisciplinary team that if pneumoperitoneum could not be achieved safely the procedure would be abandoned.
Intubation is considered the gold standard for airway protection with pneumoperitoneum as it allows tight control of ventilation parameters in patients with pre-existing respiratory impairment, as was present in this case. Caution during airway manipulation is required in all patients with OI to avoid iatrogenic injury, fracture, or cervical subluxation. Fortunately, pre-operative airway assessment was reassuring in this patient. Despite this, close attention to detail, manual inline stabilisation, and video-laryngoscopy were used to minimise the risk of harm.
Performing elective non-orthopaedic surgery when a patient has an acute fracture carries an increased risk of fracture displacement, haemorrhage, venous thromboembolism, and post-operative complications. Patients with OI have a significant fracture burden and may not be fracture free for any length of time making timing of elective surgery challenging. Accepting that there was unlikely to be an optimal time to operate, the multidisciplinary team took precautions to avoid iatrogenic injury and minimise the risk of fracture in the peri-operative period.
Elective admission to intensive care postoperatively was arranged to facilitate gradual weaning from the ventilator. There were concerns that the patient may become ventilator dependent postoperatively and require tracheostomy formation and long-term ventilation. Again, the impact of this was discussed extensively preoperatively with the patient and also the regional long-term ventilation team and paediatric intensive care specialists who have experience with OI patients. Cardio-pulmonary resuscitation (CPR) was discussed with the patient as part of the anticipatory care plan; if required this would be extremely challenging due to the patient’s body habitus, anatomy, and predisposition to fractures; however, the patient very clearly expressed his wish to receive CPR. A patient advocate was nominated by the patient should he lack capacity to make decisions during his intensive care admission particularly on life altering interventions.
This case report highlights some of the anaesthetic, surgical and critical care considerations for patients with severe OI but illustrates that with careful planning, laparoscopic surgery can be successfully performed in people with severe OI with a favourable outcome.

Comments (0)