
Remember me
Data from 1296 patients who were receiving ABP 501 (RA, n = 413; AS, n = 194; PsA, n = 418; PsO, n = 271) at the time of clinical consultation were included in this analysis. Of those, 868 (67.0%) patients were ABP 501 initiators and 428 patients (33.0%) were RP-ABP 501 switchers.
ABP 501 InitiatorsPatient demographics and clinical characteristics of the ABP 501 initiators in each disease cohort are described in Table 1. Median time from disease diagnosis to initiation of ABP 501 as the first AT was 17.2 months in PsA, approximately 22 months in both RA and AS, and 40.1 months in PsO. Most ABP 501 initiators (AS, 78.1%; PsA, 75.9%; PsO, 66.7%) received ABP 501 as a monotherapy, while in patients with RA, 72.6% received ABP 501 as a combination therapy, mainly with a conventional synthetic disease-modifying anti-rheumatic drug (csDMARD; 62.0%) (Table 1). At the time of initiation of ABP 501 treatment, the proportion of patients with RA, AS, PsA, and PsO who were classified by their physician as having moderate or severe disease was 91.4%, 92.9%, 91.7%, and 97.5%, respectively. At the time of clinical consultation (patients having been on ABP 501 for a median of 10.4–12.3 months), physicians reported that 77.1%, 63.2%, 67.8%, and 83.0% of patients with RA, AS, PsA, and PsO, respectively, were presenting with mild disease. About 85% of patients with RA and over 90% of patients with PsO were assessed by physicians to have no pain or only mild pain at the time of consultation; and the mean pain level (on a scale of 0–10) in patients with AS and PsA was 2.7 (SD 2.3) and 2.5 (SD 2.1). Overall, most physicians (RA, 89.7%; AS, 97.4%; PsA, 95.5%; PsO, 95.6%) reported being satisfied with the disease control provided by ABP 501 treatment (Table 1).
Table 1 Physician-reported patient demographics, treatment history, and clinical characteristics for patients who initiated adalimumab product (ABP 501 or reference product (RP)) as the first advanced therapyOf the ABP 501 initiators (n = 868), a subgroup of 207 patients completed the voluntary patient-reported questionnaire at the time of consultation. Most (RA, 86.3%; AS, 100.0%; PsA, 89.2%; PsO, 98.3%) reported being satisfied with the ABP 501 treatment regimen. While on treatment, the mean EQ-VAS and EQ-5D-5L utility scores were in the range 73.7–81.3 and 0.86–0.95, respectively, across disease indications (Table 2). Specifically, the five EQ-5D-5L domain utility indices (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) consistently suggested minimal impact of disease on HRQoL across all indications on the basis of patients’ self-assessment. In addition, the median overall activity impairment reported in the WPAI questionnaire was 20.0% for patients with RA, AS, and PsA and 10.0% for patients with PsO. Patients who were working reported 13.6%, 20.0%, 10.0%, and 0.0% overall work impairment in RA, AS, PsA, and PsO, respectively, and 0.0% work time missed due to their condition across all disease indications (Table 2).
Table 2 Patient self-reported measures of health-related quality of life and satisfaction for patients who initiated adalimumab product (ABP 501 or reference product (RP)) as the first advanced therapyReference Product (RP) InitiatorsA cohort of 265 patients who initiated adalimumab RP as their first AT and remained on RP therapy at the time of consultation (referred to as “RP initiators”) was included in the analysis (RA, n = 148; AS, n = 37; PsA, n = 52; PsO, n = 28). Overall, patient demographics, clinical status, satisfaction levels, and self-reported assessment of HRQoL appeared to be similar between ABP 501 initiators and RP initiators (Tables 1 and 2). However, we did observe numerical differences in treatment patterns, for example, over 70% of patients with RA received ABP 501 in combination with csDMARDs or steroids while about half of RP initiators who had RA received RP as monotherapy. Time from diagnosis to initiation of adalimumab therapy (as the first AT) was almost doubled in ABP 501 initiators relative to RP initiators among patients with AS, PsA, or PsO.
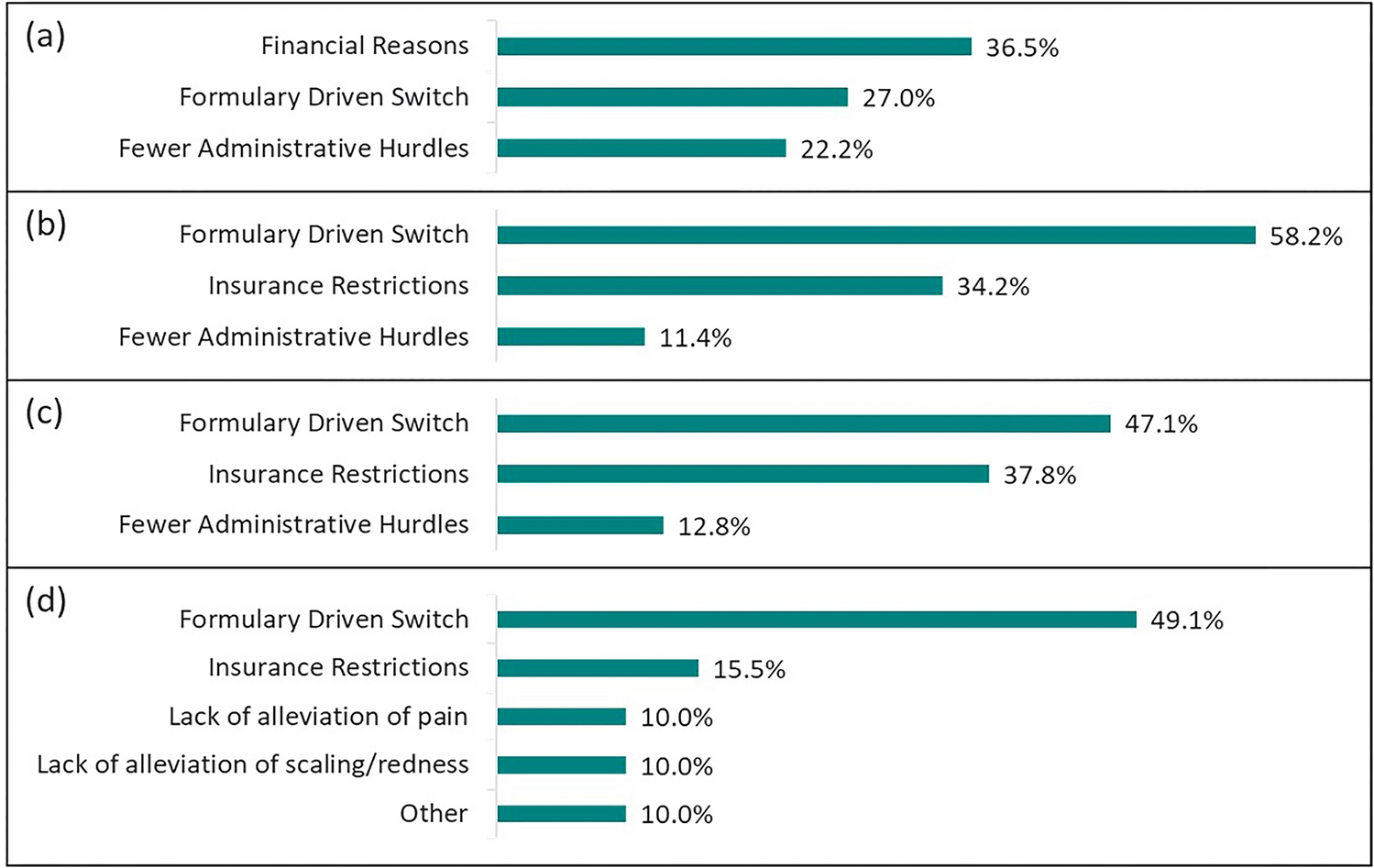
RP-ABP 501 SwitchersAmong the RP-ABP 501 switchers, the most commonly reported reasons by physicians for switching to ABP 501 were related to formulary-driven switch (RA, 27.0%; AS, 58.2%; PsA, 47.1%; PsO, 49.1%), factors relating to costs such as financial reasons (RA, 36.5%), insurance restrictions (AS, 34.2%; PsA, 37.8%; PsO, 15.5%), or fewer administrative hurdles (RA, 22.2%; AS, 11.4%; PsA, 12.8%) (Fig. 1).
Fig. 1
Top three physician-reported reasons for switching from adalimumab reference product to ABP 501. a Rheumatoid arthritis (RA) switchers, n = 63. b Ankylosing spondylitis (AS) switchers, n = 79. c Psoriatic arthritis (PsA) switchers, n = 172. d Psoriasis (PsO) switchers, n = 110. Multiple choice answer, options varied between indications
At the time of consultation, switchers had been treated with ABP 501 therapy for a median of 11.2–15.3 months across indications, following the switch from the treatment with adalimumab RP for a median of 25.9–28.6 months in patients with RA, AS, or PsO, and for a median of 12.9 months in patients with PsA (Table 3). Most switchers (AS, 86.3%; PsA, 78.6%; PsO, 71.4%) were receiving ABP 501 as monotherapy; while in patients with RA, 77.8% of switchers were receiving ABP 501 as part of a combination therapy, mainly alongside a csDMARD (58.7%). Physicians reported that the majority of switchers were experiencing mild disease (RA, 84.1%; AS, 75.0%; PsA, 81.5%; PsO, 87.5%) at the time of consultation; 87.3% of patients with RA and 95.5% of patients with PsO were evaluated by physicians to have no pain or mild pain, and for patients with AS and PsA, physician-assessed mean pain scores (on a scale ranging from 0 to 10) were 2.1 (SD 1.4) and 1.8 (SD 1.7), respectively. Overall, most physicians reported that they were satisfied with the disease control provided by current ABP 501 treatment after the switch from the RP (RA, 95.3%; AS, 98.8%; PsA, 98.3%; PsO, 93.7%) (Table 3).
Table 3 Physician-reported patient demographics, treatment, and clinical characteristics of patients who switched from adalimumab reference product to ABP 501 (RP-ABP 501 switchers)Of the RP-ABP 501 switchers, a subgroup of 111 patients completed the voluntary patient-reported questionnaires, of which 100.0% with RA, 94.7% with AS, 97.4% with PsA, and 94.9% with PsO reported being satisfied with their ABP 501 treatment regimen. Mean EQ-VAS and EQ-5D-5L score reported by patients ranged from 70.4 to 79.2 and 0.88 to 0.94, respectively, indicating an overall good HRQoL among switchers across indications (Table 4). Additionally, the five domain utility scores of EQ-5D-5L consistently suggested minimal impairment in mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Across indications, patient self-reported WPAI scores showed a median of 10.0–20.0% overall activity impairment, and among those who were working, 0.0–15.0% overall impairment, 0.0% work time missed, and 0.0–15.0% impairment while working due to their disease conditions were reported (Table 4).
Table 4 Patient self-reported measures of health-related quality of life and satisfaction for patients who switched from adalimumab reference product to ABP 501 (RP-ABP 501 switchers)
Comments (0)