The current study highlighted an increase in risk factors among patient characteristics over the past 20 years (Table 1, Fig. 1, Supplementary Material Figures S4 and S5, Table S2), while adverse events leading to discontinuation of b/tsDMARDs decreased (Fig. 2, Supplementary Material Figures S6, S7, Tables S3, and S4). Overall treatment efficacy increased for all drug classes (Fig. 5), while the treatment efficacy improved in b/tsDMARD-naïve cases and no notable improvement was observed in patients with prior b/tsDMARD experience (Fig. 5). Retention rates for IL-6Ri and CTLA4-Ig increased over time, while TNFi rates decreased (Fig. 3). However, detailed analysis revealed differences in treatment “quality” between b/tsDMARD-class (Fig. 5, Supplementary Material Figures S9 and S10), which highlighted the unmet needs; difficult-to-apply T2T patients. HAQ improvement/ normalization rates increased in all age groups, although a gap remained between younger patients and others (Fig. 7).
Statistical tests, which adjust for background factors, are valuable for providing insights to guide decision-making in cases with a wide range of treatment options. However, real-world clinical practice increasingly involves complex cases with limited treatment options, such as patients who cannot use MTX due to impaired renal function, who have substantial interstitial lung disease, or who have recurrent infections. In such cases, specific agents like abatacept are more commonly chosen. Insights from studies using statistical tests may not fully apply to these patients. Therefore, in this study, we acknowledge the limitation of not providing the defined conclusions that statistical tests may offer. Nonetheless, we performed descriptive analysis to help clinicians manage patients with significant treatment challenges.
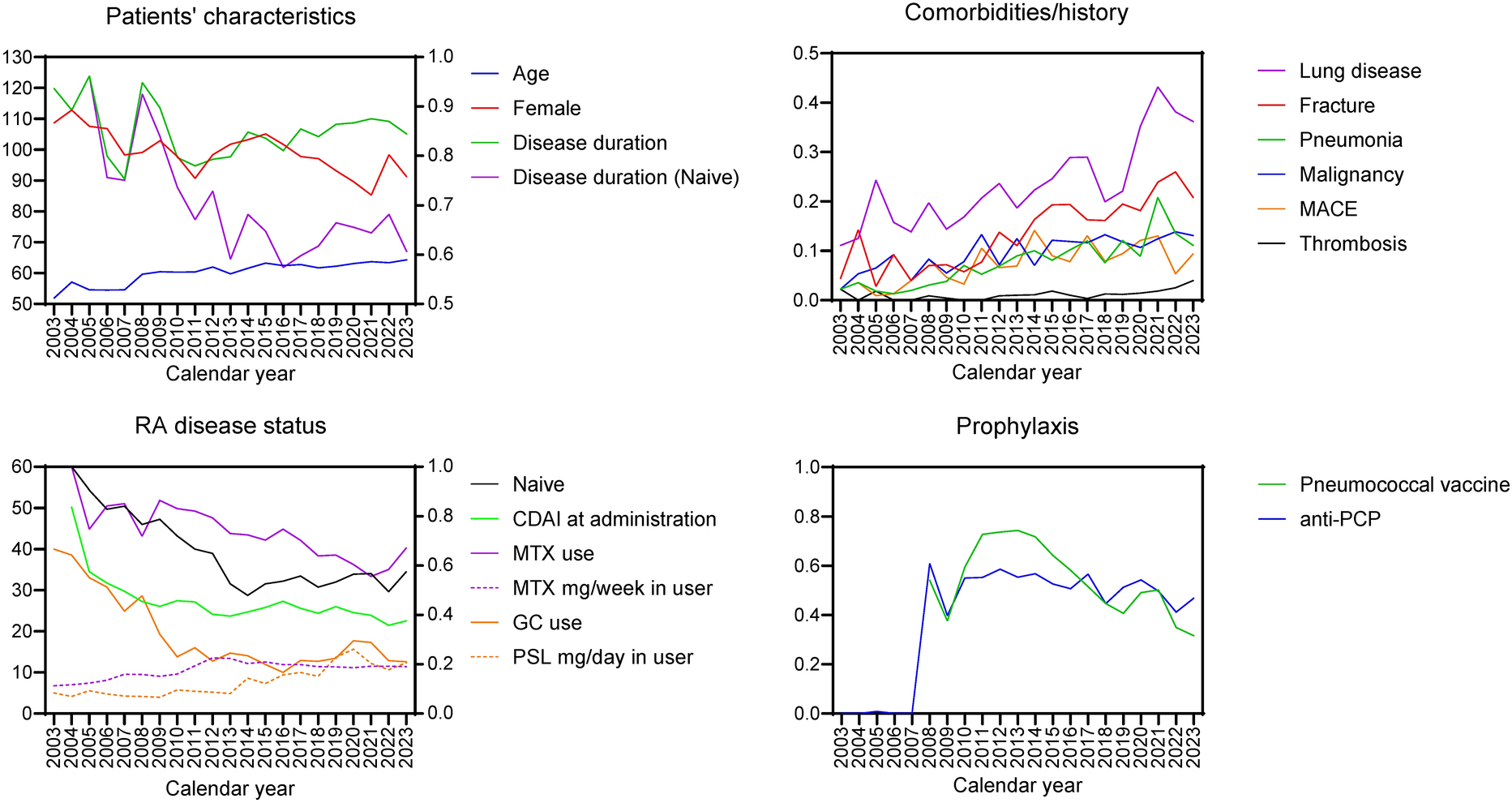
Patient risk factors increased over the past 20 years, while the use of b/tsDMARDs accelerated around 2008 and has stabilized to date (Supplementary Material Figure S2A). Moreover, treatment was initiated earlier in patients with lower disease activity (Table 1). The increase in RA complications observed in this study may be due to two key factors: an aging population and increased use of biologics, which are likely due to the inclusion of patients with more comorbidities and higher baseline risk. Although the use of MTX has gradually decreased, the dose has remained stable since 2012 (Fig. 1). This suggests that b/tsDMARDs may be more frequently administrated to MTX-intolerant patients. Even under these circumstances, the treatment efficacy increased with decreasing AEs (Figs. 2 and 5, Supplementary Material Tables S3 and S4). Thus, the study indicates an improved management of RA.
Japan became an aged society in 1998, and the subsequent acceleration of aging has been a growing concern. To maximize the benefits of b/tsDMARDs, we have focused on improving the safety and efficacy since the early 2000s. EULAR recommends vaccination for patients with autoimmune inflammatory rheumatic diseases [17]. In Japan, the 23-valent pneumococcal polysaccharide vaccine has been approved for routine vaccination of persons aged 65 years and older since 2014, with financial support from local governments. Meanwhile, FIRST registry framework has recommended pneumococcal vaccination in patients starting b/tsDMARDs since 2008. Now, more than 80% of those aged 65 years and older in FIRST registry have been vaccinated (data not shown). PCP is a common opportunistic infection with a high mortality rate. FIRST registry framework has established guidelines for PCP prophylaxis [18], and patients receive anti-PCP drugs such as trimethoprim/sulfamethoxazole accordingly (Fig. 1, Supplementary Materials Figures S4 and S5). This initiative has significantly reduced both the incidence and mortality from PCP [18]. Although routine vaccination against influenza, SARS-CoV-2, and herpes zoster are also encouraged, these vaccination histories are not collected in FIRST registry. In general, influenza vaccination is subsidized for older adults or available at personal expense, SARS-CoV-2 was free to all ages (2021–2024), and herpes zoster is self-pay; all are voluntary in Japan. Multivariate analysis from FIRST registry previously showed that even 1 mg/day of GCs in the prednisolone equivalent increased the risk of b/tsDMARD discontinuation due to infection [19]. Similarly, this study showed that MTX use was not associated with an increased risk of infections, whereas GC use was associated with infections leading to discontinuation of b/tsDMARDs, especially in older patients (Supplementary Material Figure S8). GCs can cause AEs, which complicate the management of RA [20, 21]. Both EULAR [4] and Japanese College of Rheumatology [2] recommend the use of GCs conditionally, advising rapid tapering and discontinuation. In contrast, the ACR recommends avoiding the use of GCs in RA [3]. FIRST registry framework has consistently promoted the non-use and early discontinuation of GCs. As a result, the rate of GC use declined sharply from 2003 to 2010 and has since stabilized at around 20% (Fig. 1, Supplementary Material Figures S4 and S5). Notably, the average dose of GCs has increased slightly since 2013. This may reflect a shift in the purpose of GC use from controlling arthritis to managing RA-related extra-articular complications. Unfortunately, because FIRST registry does not have comprehensive data on concomitant medication use until 2020, we cannot discuss GC tapering trends during b/tsDMARD treatment in this study. In combination with the initiatives already discussed, FIRST registry framework includes plain CT in addition to regular screening prior to b/tsDMARD administration. This strategy was effective in detecting various comorbidities, including malignancies, which likely contributed to improved patient survival [12]. CT scans also identified asymptomatic infections such as non-tuberculous mycobacteria, aspergillosis, cryptococcosis, panbronchiolitis, tuberculosis, and chronic sinusitis [12, 22]. Because these conditions could potentially worsen with b/tsDMARD treatment, patients received appropriate evaluation, treatment, or follow-up as needed [12, 22]. The incidence of infections over time has shown variability across studies [23,24,25]; however, this study demonstrated a reduction in serious infections, including opportunistic infections. These comprehensive efforts likely contributed to the decrease in infection rates over time observed in this study, despite the increasing age and comorbidities of the patient population.
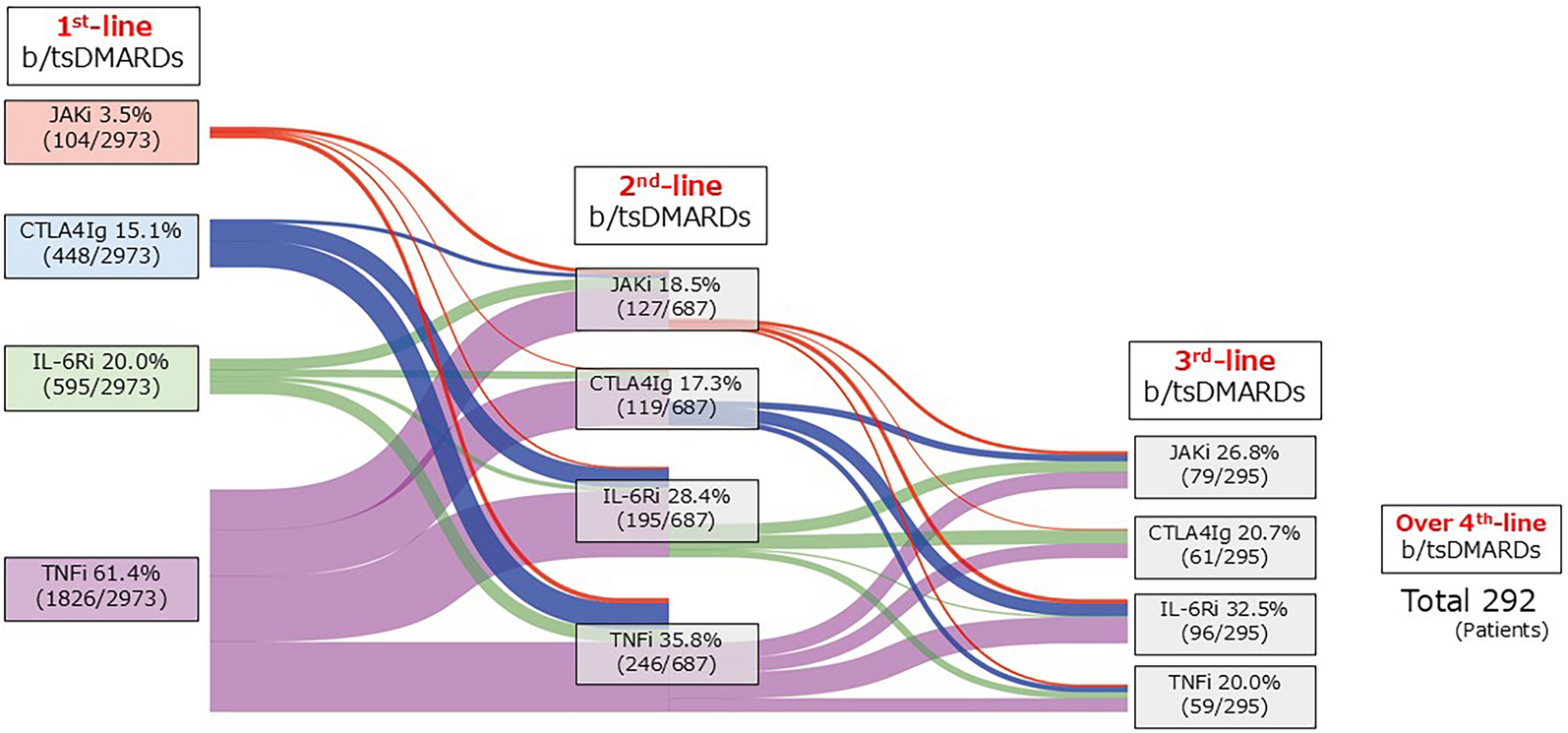
Numerous studies with statistical techniques have shown that TNFi have a lower retention rate compared to non-TNFi and JAKi [26,27,28,29,30,31,32]. Similarly, TNFi retention rates declined over eras, showing the lowest among b/tsDMARDs in Era 4 (Fig. 3). However, this study illustrated that the efficacy of TNFi improved over time, resulting in the highest remission rate in Era 4, although it was primarily discontinued due to inefficacy (Figs. 4, 5 and Supplementary Material Figure S9). Although TNFi retention rates are reportedly low in elderly patients, those using MTX with TNFi showed efficacy comparable to other b/tsDMARDs (Supplementary Material Figure S10). Thus, the younger age in the TNFi group does not explain the higher remission rates achieved with TNFi in this study. Concurrently, these data suggest that despite good efficacy, TNFi was discontinued when deemed ineffective. More importantly, the study highlighted that patients on IL-6Ri and CTLA4-Ig were more likely to remain on the treatment with a lower remission rate (Supplementary Material Figure S9). Differences in patient background (Supplementary Material Table S2) naturally affect outcomes; however, the key point is that certain population face challenges in applying T2T. TNFi was often used as the first b/tsDMARD, which may lead to early discontinuation to adhere to T2T strategies. In contrast, IL-6Ri and CTLA4-Ig were more likely to be administered to patients who were older, had a lower eGFR, and thus received less concomitant MTX. Furthermore, patients who received CTLA4-Ig appeared to have a higher risk of infection. These factors may prevent a switching from IL-6Ri or CTLA4-Ig to other drugs, such as TNFi (MTX is critical for efficacy) or JAKi (safety concerns in elderly patients [16]). However, it is important to note that the association between RA inflammation and eGFR decline [33, 34]. Although hypothetical, if patients and rheumatologists hesitate to escalate treatment because of the age, it could prolong inflammation, leading to lower eGFR, limiting MTX use, fewer b/tsDMARD options, and ultimately worse outcomes. In summary, Era 4 highlighted differences in drug retention rates, with TNFi discontinuation due to inefficacy being particularly prominent. TNFi is often switched when deemed ineffective, which may explain the lower retention rates observed in previous studies. However, given the abundant evidence of TNFi, it is worth noting that retention rates should not be the sole factor in treatment decisions. Additionally, an unmet medical need is identified: some patients continue treatment without achieving remission, suggesting that patient background may complicate T2T strategy implementation.
Functional impairment in patients with RA may not have improved over time [35, 36]. Disability-adjusted life years (DALYs) measure years of life lost (YLL) due to premature mortality and years lived with disability (YLD), reflecting the total disease burden. Age-adjusted DALYs have improved in the general population [37], whereas for patients with RA, they have worsened or remained stable [8, 38]. Considering that mortality rates among patients with RA have globally decreased over time [1, 8, 39, 40], a decrease in YLL and an increase in YLD is suggested. YLD in RA consists of comorbidities, complications, and functional impairment caused by uncontrolled RA. This study showed that discontinuation due to AEs, and "other reasons" decreased over time (Supplementary Material Table S4), suggesting that disability associated with treatment-related comorbidities and complications has decreased. However, improving functional impairment from RA inflammation is crucial to closing the DALY gap; as this aspect remains an unmet need, as highlighted by reports [36, 41, 42], and this study. While our study showed a marginal improvement in the rate of HAQ normalization, gaps remain between younger and older patients (Fig. 7). Considering that more than 75% of the general population under 75 years of age have an HAQ score of 0.38 or less [43], advances in RA management could help alleviate these challenges. Integrating these findings with the earlier discussions highlights the importance of a comprehensive approach.
Possible approaches to the issues raised in this study include: (i) considering the patients remain on treatment despite only achieving LDA, and lower response rates in patients with prior b/tsDMARD, there is a continued need for new drug development, (ii) we have recently reported factors associated with failure to achieve HAQ normalization [44]. Early and aggressive intervention should be considered in such patients, (iii) delay in treatment can cause irreversible functional impairment. Precision medicine is needed to avoid missing the window of opportunity [14], (iv) recent evidence suggests that T2T may not improve physical function alone [45]. Therefore, a multifaceted management approach is needed. Potential strategies include management of comorbidities such as depression and fibromyalgia [46, 47]; implementation of resistance training [48,49,50]; dietary therapy [50]; enhancement of self-efficacy [51, 52]; (v) management of osteoporosis [53], as fractures can lead to physical disability, especially given the low treatment rates [54]. These comprehensive approaches will be essential for effective RA management.
This study includes certain limitations. While this study confirmed unmet needs reported worldwide, whereas the findings may not be directly applicable to global populations. Furthermore, potential biases in patient selection must be considered when interpreting the results. Additionally, this descriptive analysis does not establish causation. The observed reduction in AEs could be due to people being biologically "younger" today. However, it is clear that older patients still experience greater physical disability. The structure of the Japanese healthcare system, which allows patients to be treated at multiple hospitals, can lead to data gaps if follow-up visits are missed. This issue is particularly important for deceased patients, as FIRST registry can only capture deaths that occur at participating sites. For patients who discontinue visits, it is not possible to distinguish between patient-initiated discontinuation and death, resulting in incomplete mortality data and preventing this study from analyzing mortality outcomes. Nevertheless, as discussed in this paper, numerous studies have documented a decrease in mortality in patients with RA.

Comments (0)