
Remember me
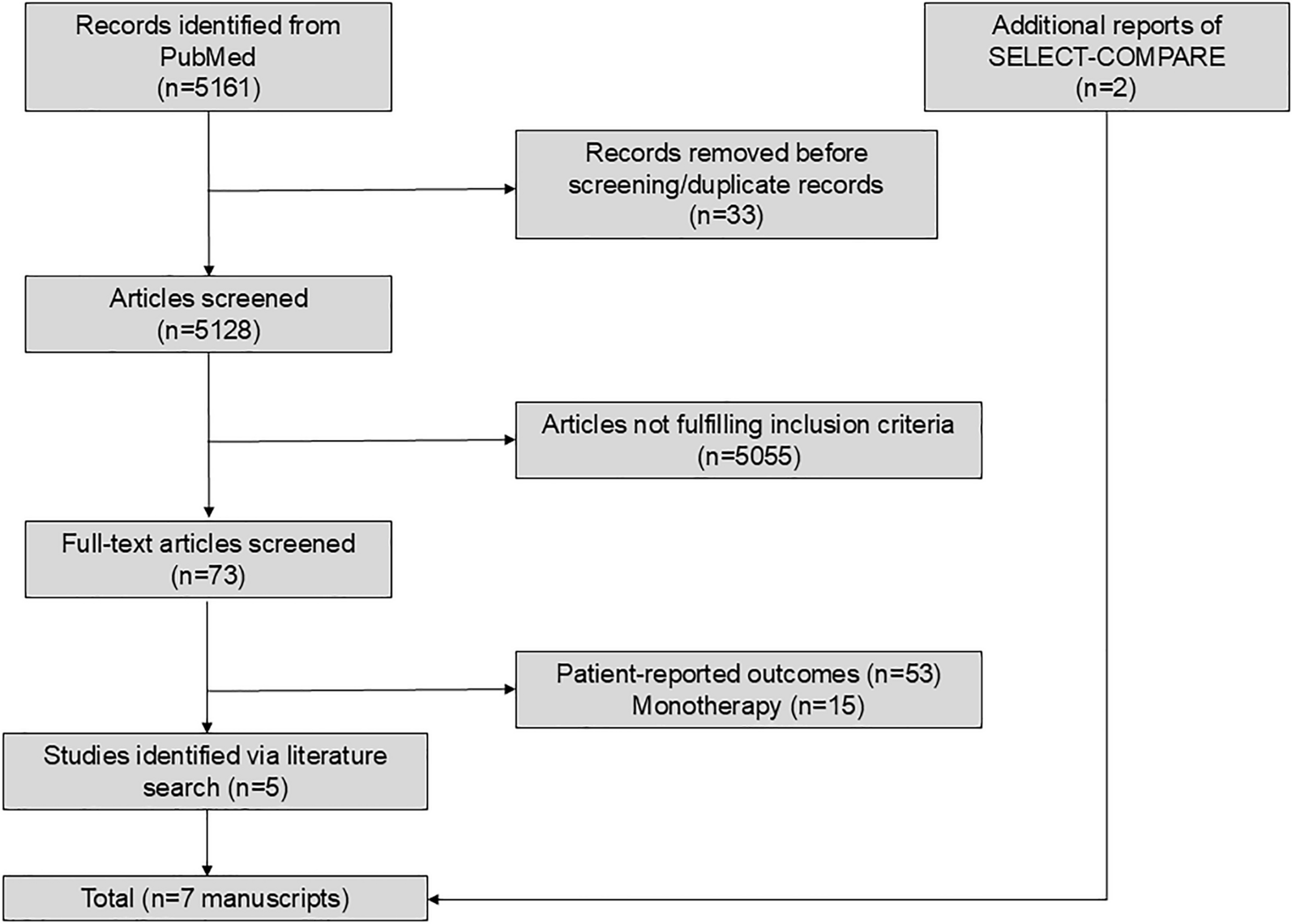
A total of 5161 publications were identified from the systematic literature search. After removing duplicates, 5128 articles remained, and 73 articles were identified as fulfilling the eligibility criteria after a review of titles and abstracts. After screening the full text of the 73 articles, five studies were included in evidence synthesis [7, 18,19,20, 22]; a study by van Vollenhoven was considered for inclusion [25], but it did not include sufficient data to include in meta-analysis of the endpoints presented in this report. Two additional articles presenting further results from one of the studies were identified as relevant and also included [21, 26], yielding a total of seven articles in the network meta-analysis. The flow chart of literature screening is shown in Fig. 1.
Fig. 1
Flow chart of included studies
All studies enrolled patients with active RA, which was generally defined as having ≥ 6 swollen joints and ≥ 6 tender joints [7, 18,19,20,21,22, 26]; one study defined patients with active RA as having ≥ 4 swollen joints and ≥ 4 tender joints [18]. All patients were receiving background MTX, [7, 18,19,20,21,22] and the mean dose of MTX across these studies ranged from 14.9 to 17.1 mg per week [7, 18,19,20,21]; one study did not specify the background dose of MTX [22]. Baseline patient and disease characteristics of the 6933 patients from the studies are summarized in Table 1. Three references presented data from the SELECT-COMPARE study and were included in the analysis, including 12-week results, 48-week results, and a subgroup analysis [20, 21, 26]. However, patients may have received rescue treatment during the trial or were switched from placebo to upadacitinib at 26 weeks, and we could not determine the number of overlapping patients from two of these analyses. Therefore, the total number of patients whose data were used for the network meta-analysis is listed. The mean age across the groups ranged from 50 to 54 years, the majority (≥ 76%) of patients were female, and the mean duration of RA ranged from 5.4 to 10 years.
Table 1 Summary of select baseline demographics and clinical characteristics from the analyzed studiesWhile each study evaluated efficacy outcomes at different time points (e.g., 12 weeks, 24/26 weeks, and 48/52 weeks), the majority of outcome measures were evaluated at approximately 6 months (24/26 weeks) [7, 18,19,20,21, 26]. A 20% improvement from baseline in ACR criteria (ACR20) is considered a well-validated composite endpoint for assessing the signs and symptoms of RA [13], and this outcome measure was reported in all studies [7, 18,19,20, 22]. Changes from baseline in mTSS and clinical remission, defined as CDAI ≤ 2.8, were reported in most studies. Although patient characteristics differed between studies and comparisons of efficacy measures are provided in section “Network Meta-Analysis Radiographic Efficacy Outcomes”, a summary of the selected efficacy outcomes is provided in Table 2. Overall, outcome measures were generally improved compared with the active comparator or placebo across each of the studies.
Table 2 Summary of select efficacy outcomes from analyzed studiesResults of the χ2 test of heterogeneity are shown in ESM Table S2. Heterogeneity was < 40% for all endpoints analyzed except for Boolean remission at weeks 24/26, for which the I2 was 68%.
Network Meta-Analysis Radiographic Efficacy OutcomesThree studies analyzed mTSS, erosion, and joint space narrowing, including 3935 patients at 24/26 weeks and 3430 patients at 48/52 weeks [7, 19, 21]. The SELECT-COMPARE study reported data at 26 and 48 weeks [21]. The treatments evaluated included adalimumab 40 mg, baricitinib 4 mg, filgotinib 200 mg, filgotinib 100 mg, upadacitinib 15 mg, and placebo.
Modified Total Sharp ScoreAdalimumab 40 mg had the highest probability of being the treatment associated with the greatest improvement in mTSS at 24/26 weeks, followed by baricitinib 4 mg (comparisons are shown in Fig. 2a). Adalimumab 40 mg, baricitinib 4 mg, upadacitinib 15 mg, and filgotinib 200 mg achieved a robust SMD versus placebo + MTX in mTSS at 24/26 weeks (SMD with 95% credible interval excluding 0). No single treatment achieved a robust SMD over any other active comparator.
Fig. 2
Network of eligible comparisons for the modified total Sharp score (mTSS) at 24/26 weeks (a) and 48/52 weeks (b), each with network meta-analysis comparing the efficacy of all comparators. Standardized mean differences and 95% credible intervals are provided. An effect is considered to provide strong evidence when both the upper and lower limits of the 95% credible intervals are < 0. As structural outcomes were not reported in reference [18], tofacitinib is not represented here. All patients received background methotrexate (MTX)
At 48/52 weeks, filgotinib 200 mg had the highest probability of being the treatment with the greatest improvement in mTSS, followed by filgotinib 100 mg (comparisons are shown in Fig. 2B). All active comparators achieved a robust SMD versus placebo. Filgotinib 200 mg achieved a robust SMD versus adalimumab 40 mg and baricitinib 4 mg.
ErosionUpadacitinib 15 mg had the highest probability of being the treatment with the greatest improvement in erosion at 24/26 weeks, followed by adalimumab 40 mg (Fig. 3a). All active comparators achieved a robust SMD versus placebo. No single treatment achieved a robust SMD in erosion at 24/26 weeks over any other active comparator.
Fig. 3

Network of eligible comparisons of erosion at 24/26 weeks (a) and 48/52 weeks (b) and joint space narrowing at 24 weeks (c) and 48/52 weeks (d), each with network meta-analysis comparing the efficacy of all comparators. Standardized mean differences and 95% credible intervals are provided. An effect is considered to provide strong evidence when both the upper and lower limits of the 95% credible intervals are < 0. As structural outcomes were not reported in reference [18], tofacitinib is not represented here. All patients received background methotrexate (MTX)
At 48/52 weeks, filgotinib 200 mg had the highest probability of being the treatment with the greatest improvement in erosion, followed by filgotinib 100 mg (Fig. 3b). All active comparators achieved a robust SMD versus placebo. Filgotinib 200 mg achieved a robust SMD versus adalimumab 40 mg.
Joint Space NarrowingAdalimumab 40 mg + MTX had the highest probability of being the treatment with the greatest improvement in joint space narrowing at 24/26 weeks, followed by baricitinib 4 mg (Fig. 3C). Adalimumab 40 mg and baricitinib 4 mg achieved a robust SMD versus placebo.
At 48/52 weeks, filgotinib 200 mg had the highest probability of being the treatment with the greatest improvement in joint space narrowing, followed by filgotinib 100 mg (Fig. 3d). Filgotinib 200 mg and 100 mg, adalimumab, and baricitinib achieved a robust SMD versus placebo. No single treatment achieved a robust SMD in joint space narrowing at 24/26 or 48/52 weeks over any other active comparator.
Network Meta-Analysis Clinical Efficacy OutcomesAmerican College of Radiology 70Three studies analyzed ACR70 at 12 weeks (including 4689 patients), at 24 weeks (3822 patients), and at 52 weeks (2859 patients); comparators included adalimumab 40 mg, baricitinib 4 mg, filgotinib 200 mg, filgotinib 100 mg, tofacitinib 10 mg (weeks 24 and 52), upadacitinib 15 mg (week 12), and placebo (weeks 12 and 24) [7, 19, 20, 26]. Upadacitinib 15 mg had the highest probability of being the treatment achieving ACR70 at 12 weeks, followed by filgotinib 200 mg (ESM Fig. S1A). All active comparators achieved a robust odds ratio (OR) versus placebo. Upadacitinib 15 mg achieved a robust OR versus filgotinib 100 mg and adalimumab 40 mg. Filgotinib 200 mg achieved a robust OR over adalimumab 40 mg.
At 24 weeks, baricitinib 4 mg had the highest probability of being the treatment achieving ACR70 (ESM Fig. S1B), followed by tofacitinib 10 mg. All JAK inhibitors and adalimumab achieved a robust OR versus placebo. Baricitinib 4 mg achieved a robust OR versus adalimumab 40 mg and filgotinib 100 mg.
At 52 weeks, baricitinib 4 mg had the highest probability of being the treatment achieving ACR70, followed by filgotinib 200 mg. No robust comparisons between JAK inhibitors or adalimumab were observed.
Boolean RemissionTwo studies, comprising 3384 patients, analyzed Boolean remission at 12 weeks in patients receiving adalimumab 40 mg, filgotinib 200 mg, filgotinib 100 mg, upadacitinib 15 mg, and placebo [7, 20]; three studies, comprising 4146 patients, analyzed Boolean remission at 24/26 weeks and included the comparators analyzed at 12 weeks with the addition of tofacitinib 10 mg [7, 18, 20]; and four studies, comprising 3657 patients, analyzed Boolean remission at 48/52 weeks and included the comparators analyzed at 24/26 weeks with the addition of tofacitinib 20 mg + MTX [7, 18, 20, 22, 26]. Upadacitinib 15 mg had the highest probability of achieving Boolean remission at 12 weeks, followed by filgotinib 200 mg (ESM Fig. S2A). All active comparators achieved a robust OR versus placebo. Upadacitinib 15 mg and filgotinib 200 mg achieved a robust OR versus adalimumab 40 mg.
At 24/26 weeks, upadacitinib 15 mg had the highest probability of achieving Boolean remission, followed by filgotinib 200 mg (ESM Fig. S2B). No robust differences between JAK inhibitors and adalimumab were observed.
At 48/52 weeks, upadacitinib 15 mg had the highest probability of achieving Boolean remission, followed by filgotinib 200 mg (ESM Fig. S2C). Upadacitinib 15 mg achieved a robust OR versus adalimumab 40 mg.
Clinical Disease Activity Index ≤ 2.8Three studies, comprising 4689 patients, analyzed CDAI ≤ 2.8 at 12 weeks in patients receiving adalimumab 40 mg, baricitinib 4 mg, filgotinib 200 mg, filgotinib 100 mg, upadacitinib 15 mg, or placebo [7, 19, 20]; four studies, comprising 5451 patients, analyzed CDAI ≤ 2.8 at 24/26 weeks in the same treatment groups as at 12 weeks with the addition of tofacitinib 10 mg [7, 18,19,20]; and five studies, comprising 4474 patients, analyzed CDAI ≤ 2.8 at 48/52 weeks in the same treatment groups as at 24/26 weeks with the addition of tofacitinib 20 mg and without placebo [7, 18,19,20, 22, 26]. Filgotinib 200 mg had the highest probability of being the treatment to achieve CDAI ≤ 2.8 at 12 weeks, followed by upadacitinib 15 mg (ESM Fig. S3A). All treatments achieved a robust OR versus placebo. Filgotinib 200 mg and filgotinib 100 mg achieved a robust OR versus adalimumab 40 mg.
At 24/26 weeks, upadacitinib 15 mg had the highest probability of being the treatment to achieve CDAI ≤ 2.8, followed by baricitinib 4 mg (ESM Fig. S3B). All active comparators achieved a robust OR versus placebo. Upadacitinib 15 mg achieved a robust OR versus filgotinib 100 mg, tofacitinib 10 mg, and adalimumab 40 mg.
At 48/52 weeks, upadacitinib 15 mg had the highest probability of being the treatment to achieve CDAI ≤ 2.8, followed by filgotinib 200 mg + MTX (ESM Fig. S3C). All JAK inhibitors and adalimumab achieved a robust OR versus tofacitinib 20 mg. Upadacitinib 15 mg and filgotinib 200 mg achieved a robust OR versus adalimumab 40 mg.
Simplified Disease Activity Index ≤ 3.3Three studies, comprising 4689 patients, analyzed SDAI ≤ 3.3 at 12 weeks in patients receiving adalimumab 40 mg, baricitinib 4 mg, filgotinib 200 mg, filgotinib 100 mg, upadacitinib 15 mg, or placebo [7, 19, 20]; three studies, comprising 3822 patients, analyzed SDAI ≤ 3.3 at 24 weeks in the same treatment groups as at 12 weeks with the addition of tofacitinib 10 mg and without upadacitinib 15 mg [7, 18, 19]; and five studies, comprising 4474 patients, analyzed SDAI ≤ 3.3 at 48/52 weeks in the same treatment groups as at 24 weeks with tofacitinib 20 mg and without placebo + MTX [7, 18,19,20, 22, 26]. Filgotinib 200 mg had the highest probability of being the treatment to achieve SDAI ≤ 3.3 at 12 weeks, followed by upadacitinib 15 mg (ESM Fig. S4A). All JAK inhibitors and adalimumab achieved a robust OR versus placebo. Filgotinib 200 mg achieved a robust OR versus adalimumab 40 mg.
Baricitinib 4 mg had the highest probability of being the treatment to achieve SDAI ≤ 3.3 at 24 weeks, followed by filgotinib 200 mg (ESM Fig. S4B). All JAK inhibitors and adalimumab achieved a robust OR versus placebo.
Upadacitinib 15 mg had the highest probability of being the treatment to achieve SDAI ≤ 3.3 at 48/52 weeks, followed by baricitinib 4 mg. Upadacitinib 15 mg achieved a robust OR versus adalimumab 40 mg.
Comments (0)