Study Design and Population
This was a longitudinal cohort study of a convenience sample of 257 patients with RA treated by a group of academic rheumatologists who are primarily engaged in clinical care (not research) at one medical center in Boston MA. The study period of interest encompassed the 18 months prior to COVID pandemic (November 2018–February 2020), the 3 months of COVID lockdown (rheumatology clinic closed except emergencies, March–May 2020), and the 18 months after COVID lockdown (June 2020–September 2021).
All patients were seen by one of 11 rheumatologists participating in a separate longitudinal study of patient symptoms. Patients were included if they had been diagnosed with RA according to their rheumatologist and had at least one visit within 18 months prior to plus at least one visit within 18 months after the lockdown. Patients were excluded if they were followed for less than 1 year by the same rheumatology provider to reduce the number of one-time consultations.
This study was approved by the Brigham and Women’s Hospital (BWH) Institutional Review Board (protocol number 2021P000790).
Outcome Definitions
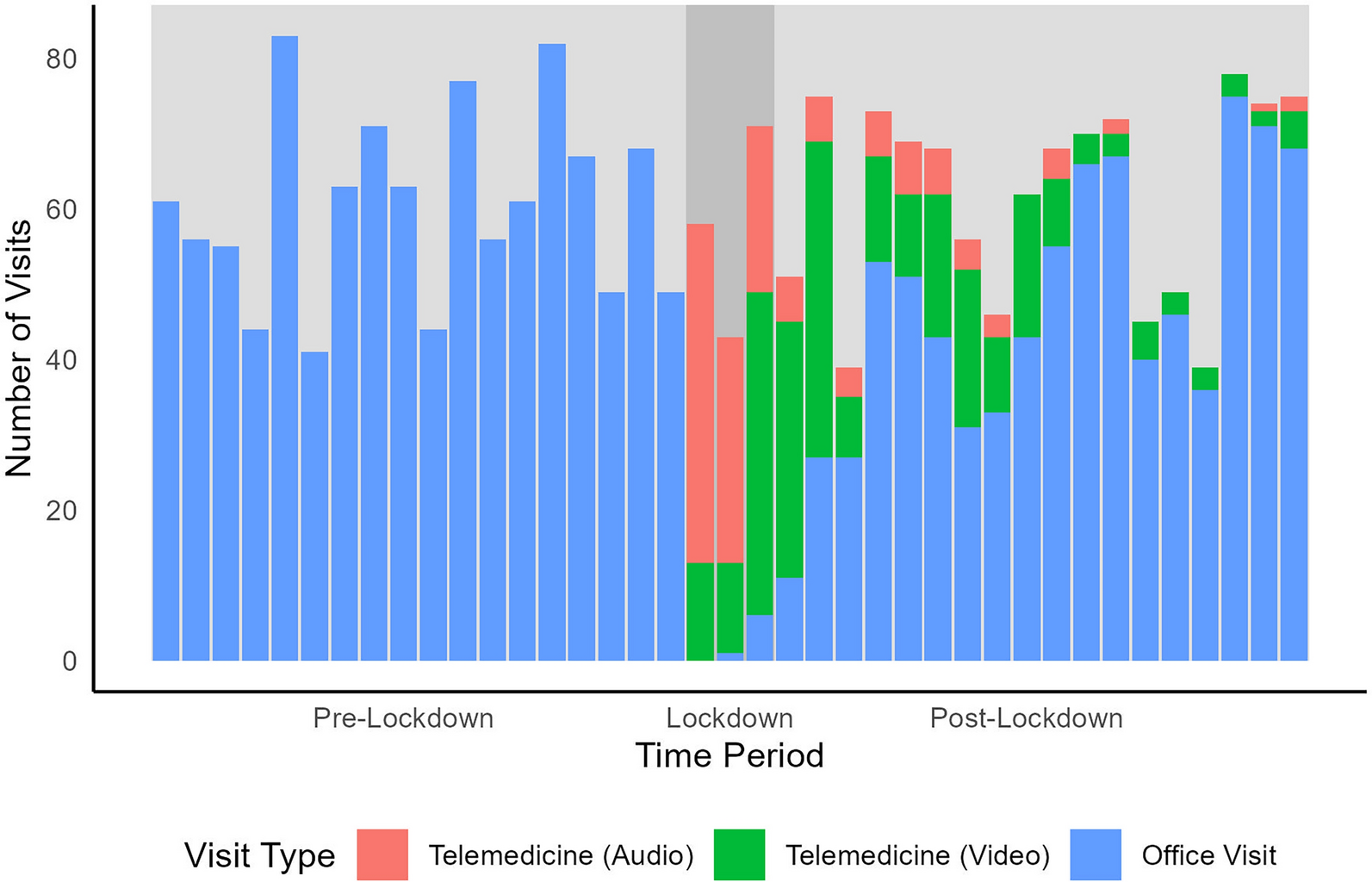
The primary outcome was the volume of in-person plus virtual visits (telephone-only or video) for RA to the patient’s primary rheumatologist. Visits were identified from the hospital billing system using specific common procedural terminology (CPT) codes entered by the specified rheumatologists during the date ranges of interest. We calculated monthly RA visit volume during the three periods of interest: pre-lockdown, lockdown, and post-lockdown. The volume of total visits and types of visits were compared across the periods of interest (see below).
The secondary outcome was annualized visit frequency per patient. In addition, the median annualized visit frequency was estimated for each rheumatologist.
Other Variables
We extracted baseline variables of interest from the medical record, using information from the 12 months prior to the start of the study period (November 2017–November 2018). These included sociodemographic (age and sex), RA characteristics (serologic status, use of disease-modifying anti-rheumatic drugs (DMARDs), use of corticosteroids, use of opioids, use of non-steroidal anti-inflammatory drugs, NSAIDs), and the specific rheumatologist seen by the patient. These variables have all been related to visit frequency in prior studies [4].
Statistical Analysis
We first derived descriptive statistics of the 257 included patient characteristics, presented as median (interquartile range, IQR) for continuous variables and frequency (%) for categorical variables. Summary statistics of the total number of outpatient rheumatology visits for the three periods were calculated, overall and by type (in-person vs. virtual). We considered visits in two ways. First, an overall visit volume by month for all 257 patients included. Second, we calculated the annualized visit frequency for each patient.
The total visit volume was plotted by month, and locally estimated scatterplot smoothing (LOESS) curves were fit to allow visual inspection of any potential trends. We used piecewise Poisson regression with knots at month 18 and 22 to estimate the trends in the count of monthly visits during the three time periods [pre-lockdown (months 0–18), lockdown (months 19–21), post-lockdown (months 22–39)]. The slope of each of the spline curves can be described as a change in the rate of visit volume per month. The 95% confidence intervals in monthly slope were estimated. No statistical testing between the slopes was pursued as there was no a priori hypothesis regarding the slopes.
We subsequently investigated the contributions of patient characteristics on visit volume by constructing linear regression models with the number of rheumatologist visits as the dependent variable. Models were constructed separately for the 18 months pre-lockdown and the 18 months post-lockdown. We also combined these periods in a secondary analysis. The models used linear mixed-effects regression models to allow for inclusion of a random effect for rheumatologist. All variables were tested in univariate models for the two separate time periods; non-significant variables were removed. Patient’s age, sex, and race were forced into all models. Additional patient characteristics considered for inclusion were comorbidity index, medication use (NSAIDs, opioids, glucocorticoids, and DMARDs), serologic status, and C-reactive protein level. Variables with p < 0.1 on univariate regression were advanced to the multivariable models. To explore the effect of clinician on visit volume, the median number of visits per patient to each rheumatologist was examined separately. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA) and R version 4.2.2 (R Core Team 2022). P values were two-sided, and statistical significance was set at p < 0.05.

Comments (0)