
Remember me
In 2001, the treatment of CML underwent a revolutionary improvement with the introduction of the first BCR-ABL-specific tyrosine kinase inhibitor (TKI), imatinib mesylate, thereby improving the survival expectancy of patients with CML [1,2,3,4]. However, the treatment remains non-curative; therefore, updated knowledge on long-term survival is essential. Several population-based studies demonstrate improvement in survival among patients with CML within the first-generation TKI era [1, 5,6,7]. Since then, more potent TKIs have been introduced, i.e., dasatinib (2006), nilotinib (2007), and bosutinib and ponatinib (2013), in case of unsatisfactory response and/or toxicity to imatinib mesylate [8,9,10,11]. Knowledge on survival among patients with CML after the introduction of a later generation of TKIs has been based on information from clinical trials, whereas data on survival in a real-world setting remain sparse [12].
This nationwide register-based study aimed to investigate the temporal 5-year survival trends among adult Danish patients with CML diagnosed in the period 1995–2017 and to compare survival among patients with CML with that of the Danish general population.
The study population included adult patients (≥18 years) diagnosed with CML between 1 January 1995 and 31 December 2017, identified using the Danish Pathology Register and the Danish National Chronic Myeloid Neoplasia Registry. The index date was defined as the first registered date of the CML diagnosis (Supplementary material, Fig. S1). Patients with CML were matched with five comparators from the Danish general population, using the Danish Civil Registration System, at the index date on birth year, sex, and comorbidity status defined as the same level of Charlson Comorbidity Index 180 days prior to the index date (or corresponding date for comparators). Charlson Comorbidity Index was calculated based on information from the Danish National Patient Register and the Danish National Prescription Registry.
The patients were categorized into four diagnostic periods based on year of diagnosis reflecting different advances in treatment: 1995–2000, 2001–2006, 2007–2012, and 2013–2017; and stratified into four groups based on age at diagnosis: 18–50, 51–65, 66–75, and >75 years. The primary outcome of this study was overall survival (OS) defined as the time from index date until death from any cause or end of follow-up (December 31 2022), whichever occurred first.
A combination of flexible parametric survival models [13], Cox proportional hazards models, and the Kaplan–Meier estimator was used to assess changes in OS during the diagnostic period 1995–2017 and compare OS among CML patients to that of the matched population, including relevant sub analyses using age standardization and stratification, respectively. For detailed information on data sources and a description of the statistical methods, see the Supplementary material.
The study included 1544 Danish patients diagnosed with CML during 1995–2017. The median age was 63 years (IQR, 48–73 years) (Fig. S1, Table S1). Clinical data were available for patients diagnosed with CML from 1 January 2010. Presentation with advanced phase CML was uncommon, with only 3.8% of patients in accelerated phase and 1% in blast phase. Most patients (86.7%) were treated with first-generation TKI while 13.3% received second or third-generation TKIs as initial therapy (Table S2).
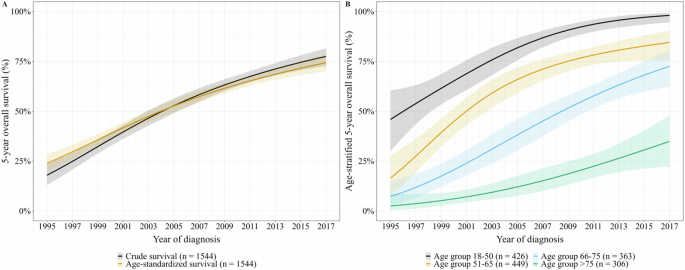
The age-standardized predicted 5-year OS improved significantly throughout the diagnostic period (p < 0.001), with an increase from 23.9% (95% CI, 19.5–28.3%) in 1995 to 74.4% (95% CI, 70.1–78.6%) in 2017 (Fig. 1A). This corresponded to an absolute increase in 5-year OS of 50.5%.
Fig. 1: Predicted 5-year overall survival (OS) according to year of diagnosis for adult Danish patients with chronic myeloid leukemia (CML).
A Crude and age-standardized 5-year OS. B Age-stratified 5-year OS. Shaded areas indicate pointwise 95% confidence intervals.
Stratified by age group, a temporal improvement for all groups was observed (p < 0.001) (Fig. 1B). Specifically, absolute improvements in 5-year OS between 1995 and 2017 for patients aged 18–50, 51–65, and 66–75 were 52.1%, 68.0%, and 65.2%, respectively. Patients >75 years at the time of diagnosis had a less favorable 5-year OS with a less notable temporal improvement of 32.4%.
The OS among patients with CML gradually approached that of the Danish general population with increasing calendar years of diagnosis. However, the OS differed between patients and matched comparators in all diagnostic periods (p < 0.001, Fig. S2). The comparison of 5-year OS between the CML cohort and the general population revealed a difference of 51.2% in 1995–2000 and 15.5% in 2013–2017 (Table S4).
OS for the latest diagnostic period (2013–2017) were stratified by age (Fig. 2 and Table S4). The difference in OS between patients with CML and matched comparators was driven by patients above 51 years of age (Fig. 2B–D). No difference in OS was found between patients with CML aged 18–50 years and their matched comparators (p = 0.353, Fig. 2A).
Fig. 2: Overall survival (OS) curves estimated using Kaplan–Meier for Danish patients with CML and a matched Danish general population in 2013–2017 stratified by age.
A 18–50 years, B 51–65 years, C 66–75 years, and D > 75 years. Shaded areas indicate pointwise 95% confidence intervals.
This Danish nationwide population-based cohort study investigated temporal changes in OS among 1544 patients diagnosed with CML in a real-world setting over the past two decades. The study demonstrated a continued increase in 5-year OS for patients with CML of all ages, even after the introduction of second and third generations of TKIs. However, the study also demonstrated an excess mortality among patients with CML compared with the general population. The survival gap was seen among patients above 50 years of age, whereas the OS of younger patients corresponded to the OS of the general population.
Former research has emphasized temporal improvements in survival among patients with CML after the introduction of first-generation TKIs. A Swedish population-based study showed a continued improvement in survival from 1973 to 2008 [1]. These findings were confirmed in a population-based study from the Netherlands showing a significant improvement in 5-year survival from 1989–2000 to 2007–2012 [5]. The current study demonstrated a continued increase in age-standardized 5-year OS during an extended period from 1995–2017. Various factors may have contributed to this considerable improvement, including enhancements in diagnostic methods and monitoring of CML, as well as treatment options. It is evident that survival was increased by the introduction of the first-generation TKI, imatinib mesylate, in 2001. The advancement in OS continued throughout the following years during the TKI era; between 2001–2006 and 2007–2012, the 5-year OS improved by 22.8% in agreement with the findings in the Dutch study in resembling periods [5]. Availability of second-generation TKIs may have affected the improvement in OS during this period. However, in the current study, data regarding treatment was limited as data was not available prior to 2010, thus it was not possible to examine the correlation directly.
Several population-based studies have stated that the survival among patients with CML approaches that of the general population [5, 12, 14, 15]. A Swedish study investigated changes in life expectancy and loss in expectation of life after a CML diagnosis between 1973 and 2013. The study reported that patients diagnosed in 2013, on average, could expect a three-year reduction in life expectancy compared with the general population [14].
Other studies found that survival among patients with CML has approached that of the general population [5, 12]. Collectively, the results in these studies are in line with the trends in the present study. Despite a remarkable improvement in 5-year OS among patients with CML during the TKI era, the survival has not yet matched that of the general population. A higher mortality rate in the initial years after diagnosis of CML was the primary cause of the difference in OS, although divergence of survival seems to persist several years after. Additional analysis showed that higher age was a contributing factor to the excess mortality observed in the period 2013–2017. Our study found no difference in survival between patients with CML aged 18–50 years and their matched comparators within the last diagnostic period, showing that the survival among the younger patients matched that of the general population.
The strength of this study derives from the use of well-established and long-running nationwide population-based registers. The Danish healthcare system is government-funded, and all patients with CML are diagnosed and treated in public hospital departments of hematology according to national guidelines. In relation to this, clinicians and pathologists are legally obligated to report data on CML, resulting in registers of high coverage and complete follow-up. Furthermore, the study design limits the influence of selection bias, as we included all patients diagnosed with CML from 1995–2017, thus assembling a representative CML cohort for the examination of a general trend in survival. The nationwide Danish Civil Registration System ensures complete follow-up of all participants. Limitations of the study mainly pertain to limited information on treatment, as this data is not available prior to 2010. Thus, the assumptions to explain the temporal changes in survival are based on the year of approval of different TKIs.
In conclusion, during the last two decades, the 5-year OS among Danish patients with CML has improved significantly, possibly driven by the advent of TKIs. The increase in survival was most notable in the younger patients, although a significant improvement was observed for all age groups. The findings of the study provide optimism for patients with CML, as they can expect survival rates approaching those of the general population. However, there remains room for further clinical improvements, since excess mortality is still evident. Additional research is necessary to determine the underlying causes contributing to mortality in patients with CML, thus identifying potential areas for intervention.
Comments (0)