
Remember me
Fifty-seven subjects with untreated follicular lymphoma were enrolled from December 2017 to November 2020 and all 57 were eligible. One eligible subject withdrew consent prior to starting treatment. Fifty-six eligible and treated subjects were included in safety and efficacy assessments. Subject characteristics are listed in Table 1. Ninety-six percent of subjects were high tumor burden by GELF.
Table 1 Baseline Characteristics.Figure 2 shows patient flow through the study. Eleven subjects did not complete 6 cycles of VEN-OB and 11 did not start maintenance therapy. Only 5 subjects completed all 12 cycles of maintenance therapy (Supplement Table 1). Reasons for discontinuation are presented in Fig. 2.
Fig. 2: Subject flow diagram.
Flow of all subjects that signed consent through the course of study including reasons for stopping protocol treatment early.
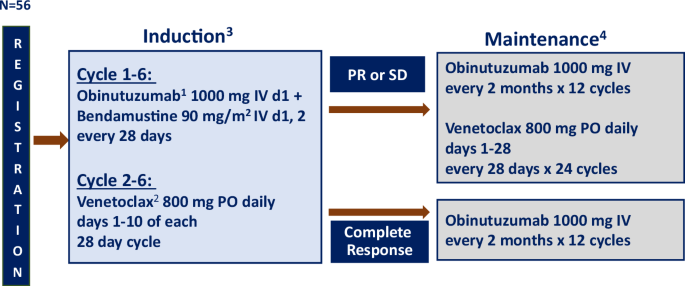
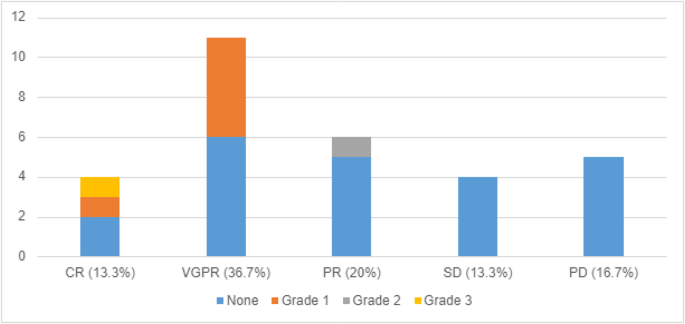
Efficacy assessmentsThe observed CR rate with VEN-OB induction was 73.2% (41/56), achieving the primary endpoint. ORR was 92.9% (52/56) with 11 subjects (19.6%) achieving PR, and 1 subject (1.8%) achieving stable disease (SD). Of the 12 patients with PR or SD, 4 (33.3%) did not undergo maintenance due to investigator discretion (n = 1), AE [n = 2], or disease progression [n = 1], and 1 (8.3%) underwent maintenance but stopped treatment prior to disease assessment. Thus, 7 (58.3%) were evaluable for improvement in response with maintenance; 3 of these 7 received obinutuzumab only due to prior AEs with VEN and 4 of the 7 received both obinutuzumab and VEN maintenance. Three of these 7 converted from PR to CR, and the single patient with SD converted to PR. The 4 subjects with deepening response were evenly split between receiving obinutuzumab only (n = 2) and obinutuzumab and VEN (n = 2) maintenance.
At the time of data cut-off, median (Q1, Q3) follow up was 34.9 months (29.3, 43.6) and all subjects had completed planned 2 year follow up. The estimated 2-year (90% confidence interval) PFS and OS were 87.5% (75.3, 93.9%) and 94.6% (86.7, 97.9%). (see Fig. 3).
Fig. 3: Survival curves.
Progression free (A) and Overall Survival (B) for all patients treated on protocol (N = 56); Median (Q1,Q3) follow up of 34.9 months (29.3mo, 43.6mo); 2 year PFS (90% CI) was 87.5% (75.3%, 93.9%) and 2 year OS (90% CI) was 94.6% (86.7%, 97.9%).
Adverse eventsTable 2 lists Treatment Related Adverse events (TRAEs) occurring in ≥10% of subjects during induction and maintenance. Of note, laboratory TLS was observed in 8 of 21 (38.1%) subjects at planned interim analysis, when VEN was administered with cycle 1. All episodes of TLS were laboratory; no clinical TLS was seen [15]. After amending the protocol to initiating VEN with C2, no TLS was identified in the 35 additional treated subjects.
Table 2 Incidence of adverse events during induction or maintenance occurring in ≥ 10% of subjects.All but 1 subject experienced a TRAE of any grade and 83.9% (90% CI: 73.6; 91.4%) (47/56) developed a Grade ≥ 3 TRAE during induction therapy. Excluding the expected AE of lymphopenia, Grade ≥3 TRAE of any grade was 75% (42/56) during induction therapy. Serious adverse events (SAE) occurred in 32 (57.1%) unique subjects during induction. Of the 34 subjects who entered maintenance therapy, 14.7% (n = 5) did not experience any TRAE while 85.3% (90% CI: 71.5, 94.0) (29/34) developed Grade ≥ 3 TRAE and 16 (47.1%) unique patients experienced a SAE.
Four atypical infections were noted at the end of induction or during maintenance therapy. One subject developed PJP at the end of treatment, prior to maintenance therapy and subsequently developed a Grade 5, cytomegalovirus (CMV) encephalitis event thought to be related to treatment. At the time of this event, the study was modified to monitor for CMV and mandate PJP prophylaxis and anti-viral prophylaxis per institutional standards. No additional CMV infections were identified following the amendment. Another subject developed a Grade 3 PJP event during cycle 3 of maintenance obinutuzumab while on PJP prophylaxis (Bactrim) for 6 months. One subject developed a Grade 4 BK virus nephropathy after cycle 6 of maintenance obinutuzumab, which resulted in end stage renal disease and chronic dialysis. Finally, a Grade 5 myocarditis event, suspected, but not proven to be viral related, occurred in a participant after 8 cycles of maintenance obinutuzumab and 18 months of maintenance venetoclax. After the Grade 5 myocarditis event occurred, all subjects had finished induction and only 7 remained on maintenance. After discussion with the study team, it was decided to discontinue maintenance therapy for all study participants (see Fig. 2).
Immunohistochemistry analysisFormalin fixed paraffin embedded (FFPE) tumor specimens were available for 47 of 56 study participants. IHC data was missing in 3 for BCL-xL and 1 for MCL-1. Thus, the effective sample size for BCL-2, BCL-xL, and MCL-1 analysis was 47, 44, and 46, respectively. As expected, the vast majority of tumor samples showed robust BCL-2 expression by IHC, with 94% having an H-score of ≥80% (median 210%; range 0–297%). BCL-xL was also highly expressed, with 70% of samples having an H-score of ≥80% (median 106.5%; range 0–180%). Meanwhile, MCL-1 staining was more often minimal to absent (median 11.5%; range 0–189%). (see Fig. 4). H-score correlations were weak between the three proteins. Spearman’s correlation between BCL-2 and BCL-xL was -0.20; between BCL-2 and MCL-1 was -0.19; and between BCL-xL and MCL-1 was 0.40.
Fig. 4: H-Score distribution for all anti-apoptotic proteins.
Immunohistochemistry derived H-Score for antiapoptotic proteins including BCL-2 (n = 47), BCL-xL (n = 44) and MCL-1 (n = 46) on pre-treatment formalin fixed, paraffin embedded diagnostic samples. There was robust expression of BCL-2 and high expression of BCL-xL. Minimal to no expression of MCL-1 was seen.
Correlations with clinical outcomes (CR rate, median PFS, and 2 year OS) were assessed for five different H-scores, including those of the individual antiapoptotic proteins (BCL-2, BCL-xL, and MCL-1) as well as the summed H-score for the non-BCL-2 proteins (BCL-xL and MCL-1) and the summed H-score for all antiapoptotic proteins combined (BCL-xL, MCL-1, and BCL-2) (see supplement Table 2). There was no correlation seen between CR rate for the 5 different assessments, possibly due to the high overall CR rate observed in this study. Further, as described above, BCL-2 and BCL-xL were both expressed at high levels in the vast majority of tumors, thereby limiting the variability between samples. Finally, our immunohistochemical analysis employed a single antibody to assess BCL-2 expression, and there remains the potential for false negative staining due to the impact of somatic hypermutation on the BCL2 locus and resultant loss of antibody recognition [16].
Cut-offs for high and low H-scores were non-linear for BCL-xL, MCL-1 and the sum of all antiapoptotic proteins. Associations with median PFS were seen for the H-scores of MCL-1 and the sum of all antiapoptotic proteins, utilizing the optimal (non-linear) cut-offs. For both values, higher H-scores were associated with longer median PFS (see supplemental Table 2). Associations with 2-year OS were observed for the sum of all antiapoptotic proteins H-score using both the median cutoff and the optimal cut-off. In both instances, higher H-scores were associated with improved 2-year OS (see supplemental Table 2).
Comments (0)