
Remember me
MRD monitoring has increasingly emerged as a pivotal dynamic biomarker in acute myeloid leukemia (AML), offering additional prognostic value beyond baseline disease genetics and standard response assessment [1, 2]. While MRD evaluation using reverse-transcription quantitative polymerase chain reaction (RT-qPCR) and multiparametric flow cytometry (MFC) has been well established in patients undergoing intensive chemotherapy [3], its role in low-intensity venetoclax-based regimens remains less clearly defined. Although recent work has separately demonstrated the prognostic significance of MFC [4,5,6] and NPM1-based RT-qPCR in NPM1-mutated AML patients receiving venetoclax plus hypomethylating agents [7], further evidence is needed to establish real-life impact of MRD in this clinical setting. Our multicenter retrospective analysis, conducted within the Spanish CETLAM Group, was designed to address this gap. Here, we evaluated the impact of MRD response assessed according to the 2021 European LeukemiaNet (ELN) recommendations on survival outcomes in a real‐world cohort.
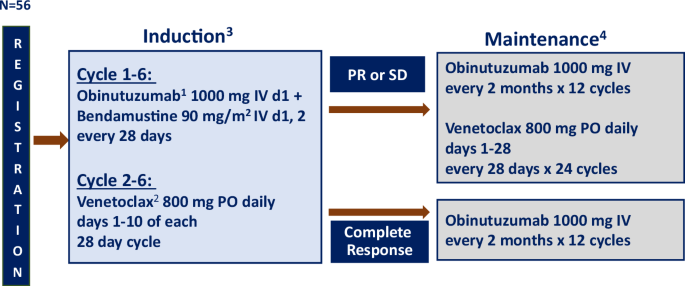
In our study, we analyzed retrospectively 99 patients, diagnosed with AML according to the ICC 2022 [8] and WHO 5th [9] and stratified according to the latest ELN risk classifications [10, 11], who achieved a morphological complete response after receiving at least two cycles of venetoclax in combination with hypomethylating agents (VenHMA) (Supplementary Fig. 1). Adult patients were treated between March 2019 and July 2024 across six centers within the Spanish CETLAM Group.
Treatment consisted of standard schedule of venetoclax (target dose of 400 mg per day) in combination with either azacitidine or decitabine, and the cohort included both newly diagnosed and relapsed/refractory patients. MRD assessment followed ELN 2021 criteria [3], and was performed using a decentralized protocol with harmonized cutoffs across centers. For those patients with molecular markers, namely NPM1 mutation or core-binding factor fusion transcripts (i.e., RUNX1::RUNX1T1 or CBFB::MYH11), MRD was assessed using RT-qPCR with a sensitivity threshold of 0.01%. In patients lacking these targets, MRD was measured by MFC with a sensitivity threshold of 0.1%, employing a panel of markers including CD34, CD117, CD45, CD33, CD13, CD56, CD7, and HLA-DR. Primary endpoint was to analyze the prognostic value of MRD in overall survival (OS), while leukemia-free survival (LFS) and the correlation of MRD response with other variables were the secondary endpoints.
We used χ2 (Fisher’s exact test when indicated) and Wilcoxon’s rank-sum tests to compare categorical and continuous variables, respectively. MRD impact on OS and LFS was assessed as a time-dependent variable using the Mantel–Byar method (displayed with Simon–Makuch curves) and landmark Kaplan-Meier analysis. LFS was calculated from date of complete remission until morphological relapse, death, or last follow-up. We performed univariate analyses with log-rank test and Cox proportional hazards’ model for multivariate analysis.
Baseline characteristics and response characteristics are shown in Table 1. Median age was 74 years (IQR: 72–78), with women comprising 51.5% of the patients. Most patients received VenHMA as frontline therapy, while a smaller subset presented as relapsed or refractory. Patients received VenHMA as frontline therapy (ND) (n = 77, 78%) or in a relapsed/refractory (R/R) (n = 22, 22%) status. AML with myelodysplasia-related (MR) features were the most frequent diagnosis (n = 44, 44.5%, including MR gene mutations, (38.4%), and cytogenetic abnormalities (6.1%)), followed by mutated NPM1 (33.3%), and mutated TP53 (13.1%)). According to the ELN 2024 genetic risk classification for lower-intensity therapies, 51.5% of the patients were classified in the favorable risk group, 19.2% in the intermediate, and 17.2% had an adverse risk. Female sex (p = 0.01), patients diagnosed with AML with mutated NPM1 (p = 0.04) and younger patients (p < 0.001) presented a higher MRD response rate.
Table 1 Baseline characteristics, response characteristics and outcomes of all patients.Median number of treatment cycles was 6 (range 2–34). Complete response (CR) rate was 54.5%, 38.4% of the patients achieved complete response without hematological recovery (CRi) and a 7.1% of the patients a morphologic leukemia-free status (MLFS). Median cycles to achieve first response were 1 (range 1–8). Patients who achieved CR reached more frequently a MRD response during follow-up (63.5% vs. 44.7%, p = 0.01) (Supplementary Fig. 2).
MRD during follow-up was assessed using MFC in 63 patients, and RT-qPCR in 36 patients. Overall, MRD response rate was 52.6%. Median number of cycles to MRD response was 2 (range 1–14). MRD response rates at 2, 4, 6 and 10 cycles were 25.2%, 38.4%, 45.5% and 50.5% respectively. Individual MRD response rates using MFC and RT-qPCR were 42.9% and 69.4% (Supplementary Fig. 1). With a median follow-up of 12 months, 46.5% of patients ended treatment due to relapse, while due to myelotoxicity occurred in 6.1% of the patients.
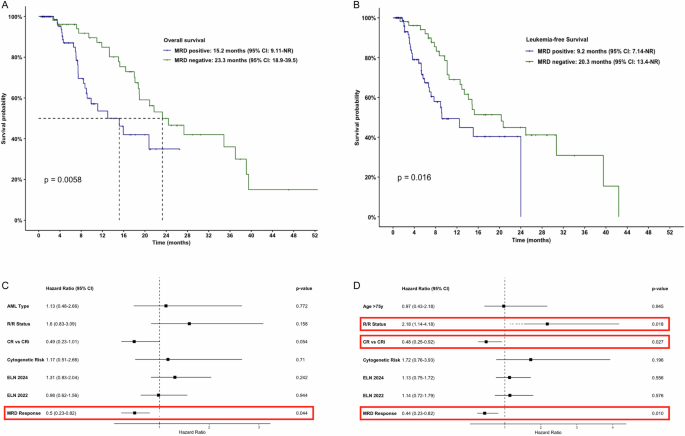
Median OS and LFS of all patients were 18.8 (95% CI: 15–24.4) and 12.5 months (95% CI: 9.18–20.3), respectively. MRD response had prognostic value for both OS and LFS (Fig. 1A, B) with a median OS of 23.3 months (95% CI: 18.8–39.5) vs. 15.2 months (95% CI: 9.11–NR), p = 0.006, and median LFS of 20.3 months (95% CI: 13.4–NR) vs. 9.2 months (95% CI: 7.1–NR), p = 0.01) and landmark analysis after 2 cycles in both cases (p < 0.0001, Supplementary Fig. 3). No other landmarks were significant for outcomes (e.g., 4-cycle landmark analysis for OS: p = 0.41).
Fig. 1: Survival outcomes by MRD Response.
Overall survival (A) and Leukemia-free Survival (B) of all patients by MRD Response estimated using the Mantel–Byar method (Time-dependent variable) (Simon–Makuch Graph). Multivariate analysis for Overall Survival (C) and Leukemia-free Survival (D). AML Acute Myeloid Leukemia, R/R Refractory/Relapsed, CR vs. CRi Complete Response versus Complete Response versus Complete Response without Hematologic Recovery or Morphologic Leukemia-Free Status, ELN European LeukemiaNet, MRD Measurable Residual Disease, CI Confidence Interval.
MRD response was significant regardless of the MRD assessment technique. I patients with measured by RT-qPCR, OS (NR vs. 9.2 months, p = 0.006) and LFS (42 vs. 9 months, p = 0.04. Supplementary Fig. 3) were longer in MRD responders. Analysis with MFC also showed prognostic value for OS (18.9 vs .7.4 months, p < 0.001) and LFS (14.8 vs. 5.3 months, p < 0.001) (Supplementary Fig. 4).
Additional prognostic factors for survival were AML with NPM1 mutation, with better LFS (20.3 months vs. 10.5 months, p = 0.02) and a trend for better OS (23.3 months vs. 16.4 months, p = 0.06) compared to other AML subtypes, while those receiving VenHMA as frontline therapy showed a trend for better OS (18.9 months vs. 11.9 months, p = 0.09) and LFS (14.1 months vs. 7.8 months, p = 0.06). No other prognostic factors were identified in univariate analysis, including ELN 2022 risk, lower-intensity adapted ELN 2024 risk, or TP53 mutational status.
The independent prognostic value of MRD for OS (HR: 0.50, 95% CI: 0.23–0.82; p = 0.04) and LFS (HR: 0.44, 95% CI: 0.23–0.82; p = 0.01) was confirmed in the multivariate analysis. In addition, disease status at baseline (R/R vs. frontline, HR: 2.18, 95% CI: 1.14–4.18, p = 0.008) and response type (CR vs. CRi (HR: 0.48, 95% CI: 0.25–0.92, p = 0.027)) also emerged as independent prognostic factors for LFS (Fig. 1C, D).
These findings underscore the clinical value of serial MRD monitoring in the context of VenHMA treatment. Unlike intensive chemotherapy regimens, where early MRD responses are commonly observed, VenHMA-treated patients exhibit a more gradual response kinetics. Thus, only 25% of patients had achieved MRD response by the end of cycle 2; however, with continued therapy, the cumulative MRD response rate increased to above 50%. This delayed response suggests that a single, isolated early MRD assessment may underestimate the response depth, making extended monitoring essential for predicting long-term outcome. Our findings align with recent evidence in this setting and re reflected ine the latest ELN-DAVID MRD recommendations for lower-intensity treatments [12].
Importantly, the prognostic impact of MRD was observed regardless of the assessment method used. In patients evaluated by RT-qPCR—primarily those with NPM1-mutated AML—the survival differences between MRD-negative and MRD-positive patients were especially pronounced, underscoring the higher sensitivity of molecular techniques, with a detection threshold 1 log below that established for MFC-based assessment. This observation confirms that the clinical relevance of MRD testing depends on both the sensitivity of the assessment method and the kinetics of the AML subtype also in the setting of low-intensity therapy, similarly to what it has been observed in patients treated with standard chemotherapy [13, 14].
These findings have significant clinical implications. Stratifying patients based on MRD status provides a powerful tool for identifying those at increased risk of relapse who might benefit from early therapeutic intervention. Furthermore, integrating MRD monitoring into routine clinical practice in the context of low-intensity AML therapy may allow a more dynamic treatment adaptation, with the ultimate goal to improve patient outcomes, although current options after VenHMA failure remain highly limited [15].
Despite the strengths of our study, several limitations must be acknowledged. The retrospective nature of the analysis inherently introduces potential biases, and the decentralized MRD assessment, especially relevant using MFC, may cause variability in sensitivity and interpretation across centers. Additionally, the heterogeneity of the disease status, since we included ND-AML and R/R AML patients, could have had an influence on outcomes. Nevertheless, the consistency of the survival benefit associated with MRD negativity across various subgroups reinforces the strength of our findings.
We conclude that MRD response, evaluated accordingly to the ELN-MRD 2021 recommendations, holds significant prognostic value for both OS and LFS in patients treated with VenHMA in real-life clinical practice. These findings underscore the importance of MRD monitoring also in the context of low-intensity AML therapy as an essential prognostic factor, and warrant the exploration of preemptive interventions based on MRD within a well-designed research framework.
Comments (0)