
Remember me
First, we examined the genetic and pathological features of CrF. Comprehensive genomic analysis using the K-means clustering method revealed a set of genes, known as Cluster A genes, expressed in the mesentery of patients with CD. These included immune response, lymphocyte activation, and immune regulatory genes, suggesting that the immune response was highly activated (Supplementary Fig. 1A; Table 1).
Table 1 Results of RNA sequencing analysisNext, we investigated the histopathological features of CrF compared to those of the control. In CrFs, cell aggregation and infiltration were observed in the intestinal wall, breaking through the serosa (Fig. 1C; left and middle panels). In addition, the connective tissue within the adipose tissue was thickened due to surrounding cell clusters (Fig. 1C; right). On the other hand, in the control mesentery, only a small number of cells were found, with no evidence of adipose tissue wall thickening or cell infiltration into the mesentery (Fig. 1D). Adipocytes in CrF were round and smaller in size compared to those in the control mesentery (66.9 ± 2.1 µm vs 156.3 ± 9.5 µm; P < 0.0001; Supplementary Fig. 1B). Masson’s trichrome staining revealed substantial fibrosis in CrF, particularly in areas of adipose tissue wall thickening; however, fibrosis was rarely observed in the control mesentery (Fig. 1E-F). RNA sequence analysis demonstrated that the expression of representative fibrosis-related genes and extracellular matrix (ECM) regulators, including COL1A, COL3A, ACTA2, and PDGFB, increased in CD (Supplementary Fig. 1C). These data suggest that inflammation and significant fibrosis occur in CrF.
Characterization of human ILC subsets in mesentery of ileumNext, we examined the presence of ILCs in human adipose tissue from the subcutaneous fat, mesentery, and omentum of patients who underwent surgery for colorectal cancer. The frequency of the ILCs varied depending on the organ (Supplementary Fig. 1D). More than 60% of patients with CD have inflammatory lesions in the ileum [16]; therefore, we focused on the mesentery of the ileum in our subsequent analyses.
In the ileal mesentery analysis, CD45+ Lin− (CD3− CD11c− CD14− CD16− CD19− CD20−) CD127+ cells among SVFs were divided into CD117− CRTH2− (ILC1s), CD117− CRTH2+ (ILC2s), and CD117+ CRTH2− (ILC3s) cells using flow cytometry (Fig. 2A). The three ILC subsets from the control mesentery exhibited lymphoid morphologies similar to those of ILCs from ileal LPCs, as determined by May–Giemsa staining (Fig. 2B). Fluorescence-activated cell sorting analysis of the control mesentery revealed exceedingly small populations of ILC2s (Fig. 2C). ILC1s exhibited high expression of T-bet, a master regulator of ILC1 encoded by TBX21, whereas ILC3s showed high expression of RORγt, which is encoded by RORC and responsible for the development of ILC3s (Fig. 2D–E). These results showed that ILCs are present in relatively small amounts in human fat tissue but can be firmly classified.
Fig. 2
Characterization and analysis of ILC subsets in the human mesentery. A Gating of ILC1, ILC2, and ILC3 from human mesentery by flow cytometry. Among 7AAD− CD45+ Lin− (CD3− CD11c− CD14− CD16− CD19− CD20−) CD127+ cells, CD117− CRTH2− cells were defined as ILC1, CD117− CRTH2+ as ILC2, and CD117+ CRTH2− cells as ILC3. B Morphological analysis of ILC subsets from mesentery and ileum through May–Giemsa staining. Scale bars, 10 µm. C Frequencies and absolute cell number/g (tissue weight) of the ILC subsets among 7AAD− CD45+ Lin− (CD3− CD11c− CD14− CD16− CD19− CD20−) CD127+ cells in the control mesentery. D Flow cytometric analysis of T-bet and RORγt expression in ILC subsets purified from the ileal mesentery. Representative data of seven samples each. [E] Expression of TBX21 and RORC in ILC subsets purified from CrF by qPCR. Data are presented as means ± standard error of the mean (SEM) of seven independent donors each (*P < 0.05, **P < 0.01). Representative data from subcutaneous fat, omentum, and mesentery of the colon are shown
Distribution of ILCs in CrF and correlation with ILCs in the ileumNext, we examined how ILC subsets are altered in the CrF and whether they correlate with the ILCs of the ileum. Representative flow cytometry results for the ileal mesentery from the control, non-CrF part, and CrF part are shown in Fig. 3A. In terms of the frequency of ILCs in the ileal mesentery, ILC1s were significantly increased in the CrF part, whereas ILC2s and ILC3s were significantly decreased compared to those in the control (Fig. 3B). In terms of the number of ILCs per unit weight of mesentery, the number of ILC1s was significantly increased in the CrF part compared to the control, while the number of ILC2s did not differ between the two groups. Moreover, the number of ILC3s was decreased in the non-CrF part, but did not differ between the CrF part and the control (Fig. 3C). RNA-sequence analysis of CrFs demonstrated that the expression of ILC1-related genes, except TNFA and CCL2, was upregulated as inflammation intensified (Supplementary Fig. 1E).
Fig. 3
Correlation between ILC subsets in the human mesentery and inflammation. A Flow cytometric analysis of ILC subsets from human mesentery. Representative data from the control, CD (non-CrF), and CD (CrF) are shown. B Frequencies of ILC subsets among 7AAD− CD45+ Lin− (CD3− CD11c− CD14− CD16− CD19− CD20−) CD127+ cells depending on the state of inflammation in human mesentery. C Absolute cell number/g (tissue weight) of ILC subsets depending on the state of inflammation in the mesentery. Data are presented as mean ± SEM of 15 control donors and 17 donors with Crohn's disease (ns not significant; *P < 0.05, **P < 0.01, ****P < 0.0001). D Correlation of the frequency and absolute cell number/g (tissue weight) of ILC1s among 7AAD− CD45+ Lin− (CD3− CD11c− CD14− CD16− CD19− CD20−) CD127+ cells between ileum and mesentery. P values were obtained through Pearson's simple linear regression analysis
Representative flow cytometry results of the ileum from the control, non-CrF part, and CrF part are shown in Supplementary Fig. 2A. In terms of the frequency of ILCs in the ileum, ILC1s were increased and ILC3s were decreased in patients with CD compared to those in the control group, but no difference was found in ILC2s (Supplementary Fig. 2B). Additionally, in terms of the number of ILCs per unit weight of the ileum, the number of ILC1s increased as inflammation intensified, while ILC2s did not differ among the three groups, and ILC3s decreased in the non-CrF part (Supplementary Fig. 2C). Regarding the frequency of ILCs in the mesentery and ileum, a positive correlation was found for all ILCs, suggesting that the degrees of inflammation of the mesentery and ileum are correlated (Fig. 3D, Supplementary Fig. 2D), whereas no positive correlation was found for all ILCs regarding number per unit weight. These results suggest that ILC1s may play an important role in the pathogenesis of CD, as they are increased in both the mesentery and ileum.
Positive correlation between ILC1s and macrophages in CrFSince macrophages play an important role in adipose tissue fibrosis [17, 18], we investigated the distribution of macrophages in the mesentery and their association with ILC1s, which were increased in CrF. Among the SVFs, CD45+ Lin− (CD3− CD19− CD20− CD56−) and CD14+ HLA-DR+ cells were defined as macrophages and divided into CD163low and CD163high macrophages (Fig. 4A). As previously reported in the ileum, CD163low macrophages are inflammatory and are increased in the ileum of patients with CD [14, 19]. Macrophages in the mesentery were examined using the control, CD (non-CrF), and CD (CrF) groups, as shown in Fig. 4B. In the mesentery, the frequency of CD163low macrophages was elevated in CD compared to that in controls, and the number of CD163low macrophages per unit weight (n/g) increased with increasing inflammation (Fig. 4C). By contrast, the frequency of CD163high macrophages was higher in the control group than in the CD group. However, the number of CD163high macrophages per unit weight (n/g) was not significantly different because the overall number of macrophages increased in the CD mesentery (Fig. 4D).
Fig. 4
Macrophage subset analysis and immunohistochemistry comparison in human mesentery. A Gating of macrophages from human mesentery by flow cytometry. Among CD45+ Lin− (CD3− CD19− CD20−, CD56−) cells, CD14+ HLA-DR+ cells were defined as macrophages. Macrophages were categorized as CD163high and CD163low. B Flow cytometric analysis of macrophages from human mesentery. Representative data for five samples each from the control, CD (non-CrF), and CD (CrF) are shown. C Altered composition of CD163low macrophage subsets depending on the state of inflammation in human mesentery. Frequencies of mesentery CD163low macrophage subsets among CD45+ Lin− CD14+ HLA-DR+ cells (left) and absolute cell number/g (tissue weight; right) of mesentery. D Altered composition of CD163high macrophage subsets depending on the state of inflammation in human mesentery. Frequencies of mesentery CD163high macrophage subsets among CD45+ Lin− CD14+ HLA-DR+ cells (left) and absolute cell number/g (tissue weight; right) of mesentery. Data are presented as mean ± SEM of five independent donors each (ns not significant; *P < 0.05, **P < 0.01). E Correlation of the frequency between mesentery CD163low macrophage among CD45+ Lin− (CD3− CD19− CD20−, CD56−) CD14+ HLA-DR+ cells and mesentery ILC1s among 7AAD− CD45+ Lin− (CD3− CD11c− CD14− CD16− CD19− CD20−) CD127+ cells. F Correlation of absolute cell number/g (tissue weight) between mesentery CD163low macrophages and mesentery ILC1s. P values were obtained by Pearson simple linear regression. G Representative images of immunohistochemistry of CrF with CD68 (brown): overview of the intestine and mesentery (left), mesentery (middle), and intestinal attachment area of mesentery (right). H Representative images of double immunohistochemistory of CrF with CD3 (brown) and T-bet (red): overview of the intestine and mesentery (left), mesentery (middle), intestinal attachment area of mesentery (right). Arrows indicate CD3− T-bet+ cells. I Representative images of immunohistochemistory of control mesentery with CD68 (brown); overall view of the intestine and mesentery (left), mesentery (right). J Representative images of double immunohistochemistory of the control mesentery with CD3 (brown) and T-bet (red): overall view of the intestine and mesentery (left), mesentery (right). Arrows indicate CD3− T-bet+ cells. Scale bars, 200 µm. K Comparison of the densities of CD68+ cells/mm2 (left) and Tbet+CD3− cells/mm2 (right) between the control mesentery and CrF. Data are presented as mean ± SEM using nine pathological images from three independent donors (****P < 0.0001). L Correlation of the density/mm2 between CD68+ cells and Tbet+CD3− cells. P values were obtained through Pearson’s simple linear regression analysis
Positive correlations between CD163low macrophage and ILC1s were found for both frequency (R = 0.82, P = 0.001; Fig. 4E) and number per unit weight (R = 0.74; P = 0.006; Fig. 4F).
Next, immunostaining for CD68, a macrophage marker, and double immunostaining for CD3, a T cell marker, and T-bet, a marker for both ILC1s and T cells, were performed. CD3+ Tbet+, CD3−Tbet+, and CD68+ cells were found to be aggregated around adipocytes and at the mesenteric attachment area of CrF (Fig. 4G–H). Several crown-like structures (CLS), a phenomenon in which CD68+ cells surround adipocytes, were also observed (Fig. 4G; middle). In CLS there is ongoing inflammation, with CD68+ cells forming CLS considered to be the main inflammatory macrophages involved [20]. The images on the right in Fig. 4G and 4H show the clustering of immune cells near the intestinal tract in serial sections, suggesting that CD163low macrophage and ILC1s are present closely together.
Only a small number of immune cells, however, were found in the control mesentery (Fig. 4I–J). Counting CD3−Tbet+ and CD68+ cells and calculating their densities revealed that both cell types were increased in CrF (P < 0.0001 for both; Fig. 4K). In addition, a positive correlation was observed between the density of CD3−Tbet+ and CD68+ cells (R = 0.81, P = 0.001; Fig. 4L). These data suggest a potential interaction between ILC1s and inflammatory macrophages in CrF.
Fibrogenesis mediated by IFN-γ secreted from ILC1s in CrFTo investigate how ILC1s are involved in CrF formation, we first compared the differences in properties between ILC1s from non-CrF (ILC1 [non-CrF]) and CrF (ILC1 [CrF]) groups, noting that despite the increase in ILC1s in non-CrF group compared to the control, CrF formation was not observed. Regarding ILC1-related cytokines IFN-γ and TNF-α, no differences in TNF-α expression were observed between the two groups, but IFN-γ expression was more prominent in the ILC1 [CrF] group (Fig. 5A–C). However, subgroup analysis revealed an increase in TNF-α-positive cells in ILC1 [CrF] among patients who did not receive anti-TNF-α antibody treatment. This suggests that the majority of patients receiving anti-TNF-α antibodies may have contributed to the absence of changes in TNF-α expression levels within the tissues (P = 0.04; Supplementary Fig. 2E). We hypothesized that ILC1-derived IFNγ potentially contributes to the formation of CrFs. Thus, co-culture experiments were subsequently conducted.
Fig. 5
Functional analysis of ILC1s in CrF and clinical impact on Crohn's disease recurrence. A Expression of IFNG and TNFA in ILC1s purified from CrF and non-CrF by qPCR. Data are presented as mean ± SEM of ten independent donors each (ns: not significant; *P < 0.05). B Representative images of IFN-γ and TNF-α expression in ILC1 purified from CrF and non-CrF after cell stimulation analyzed by flow cytometry. C Expression of IFN-γ and TNF-α in ILC1s purified from CrF and non-CrF by flow cytometry. Data are presented as dots from ten independent donors (ns: not significant; ***P < 0.001). D Graphical illustration of co-culture experiments. Viable ILC1s were isolated from 15 g of CrF and cultured in the upper chamber. On the other hand, 1 × 106 of SVFs isolated from the control mesentery were seeded in the lower chamber. Neutralizing IFN-γ antibody was administered during co-culture of SVF from the control with ILC1 from CrF. E Relative mRNA expression of COL1A1, COL3A1, MINCLE, INOS, and TGFB1 in human stromal vascular fractions (SVFs) from the control of the lower chamber (ns not significant; *P < 0.05). F Graphical illustration of co-culture experiments to compare the effects of CrF-derived ILC1s and SVFs on SVFs from the control. Viable ILC1s or SVFs were isolated from 15 g of CrF and cultured in the upper chamber. On the other hand, 1 × 106 of SVFs isolated from the control mesentery were seeded in the lower chamber. CrF-derived SVFs are shown in white. G Relative mRNA expression of COL1A1, COL3A1, MINCLE, INOS, and TGFB1 in SVFs from the control cultured in the lower chamber (ns: not significant). H Kaplan–Meier estimates demonstrating the percentage of patients with recurrence-free survival after surgery for Crohn’s disease. Patients were divided into two groups: ILC1 high (≥ 80%; n = 15) and ILC1 low (< 80%; n = 19). P values were obtained using the log-rank test
Next, to investigate how ILC1s function in the mesentery, SVFs from the control (SVF [control]) were co-cultured with ILC1 [CrF] (Supplementary Fig. 3A). After 72 h, significantly increased expression of fibrosis-related macrophage genes, such as macrophage-inducible c-type lectin (MINCLE), inducible nitric oxide synthase (INOS), and TGFB1 were observed in SVF [control] co-cultured with ILC1 [CrF], compared to those cultured without ILC1s (Supplementary Fig. 3B). Moreover, the expression of collagen genes, such as COL1A1 and COL3A1, was also significantly increased in SVF [control] co-cultured with ILC1 [CrF] (Supplementary Fig. 3B).
Next, to evaluate whether IFN-γ from ILC1s promote fibrogenesis of mesentery, neutralizing IFN-γ antibody was administered during co-culture of SVF [control] with ILC1 [CrF] (Fig. 5D). After 72 h of co-culture, MINCLE, INOS, TGFB1, COL1A1, and COL3A1 were significantly increased in the SVFs [control] and ILC1 [CrF] co-culture with IgG isotype control antibody compared with those in the control group. These changes were mostly nullified by administration of neutralizing IFN-γ antibody (Fig. 5E). Since there are other IFN-γ producing cells in the mesentery, such as T and NK cells, further co-culture experiments were conducted to determine whether ILC1s are essential for fibrogenesis by comparing the effects of CrF-derived ILC1s and SVFs on SVFs from the control (Fig. 5F). There was no difference in fibrosis-related gene expression in SVFs from the control compared to that in ILC1s and SVFs from CrF (Fig. 5G). These findings indicate that IFN-γ secreted from ILC1s is essential for the fibrogenesis in CrF.
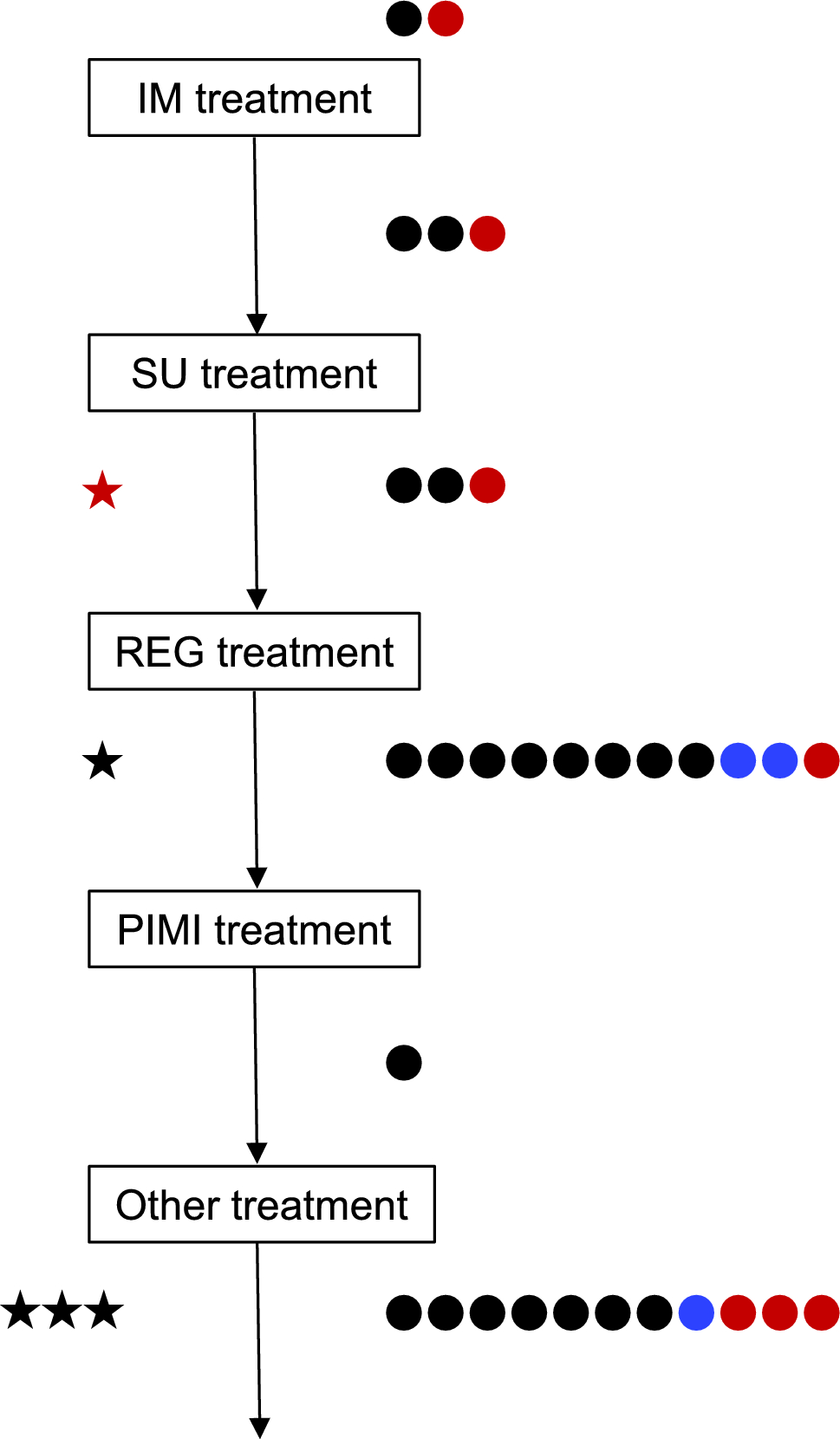
Contribution of elevated mesenteric ILC1s to endoscopic recurrence in patients with CDNext, we investigated the clinical importance of mesenteric ILC1s. Thirty-four patients with CD who underwent postoperative endoscopic examination after bowel resection were divided into two groups, one with recurrence (n = 11) and the other without recurrence (n = 23), and risk factors were assessed. As shown in Table 2, a high frequency of ILC1s in the CrF mesentery (P = 0.01) was a risk factor for early endoscopic recurrence. Conversely, there were no differences in preoperative or postoperative treatment between the two groups. Furthermore, multivariate analysis was performed, encompassing age, body mass index (BMI), preoperative serum CRP levels, and preoperative serum albumin levels, and a high frequency of ILC1 in the CrF mesentery was confirmed to be an independent risk factor (P = 0.01, odds ratio: 1.25). Next, ROC curve analysis identified a cutoff value of 80 for ILC1s in the CrF mesentery (%), and the patients with CD were divided into two approximately even groups—ILC1 high (≥ 80%; n = 15) and ILC1 low (< 80%; n = 19)—and a recurrence-free survival curve was drawn. At the median follow-up period of 520 days, the log-rank test analysis showed a significantly higher recurrence rate in the ILC1 high group (P = 0.03; Fig. 5H).
Table 2 Risk factors for postoperative recurrence of Crohn's disease
Comments (0)