In this study, we analyzed approximately one million ERCP cases using the DPC database to elucidate the current status and trends in ERCP and PEP, as well as the factors associated with the incidence and severity of PEP. Our findings revealed an increasing trend in the number of ERCP procedures per facility per month and a rising proportion of therapeutic ERCP. In contrast, the incidence of PEP and severe PEP showed a decreasing trend. Regarding PEP prevention, the use of rectal NSAIDs increased, while the use of PIs declined. Notably, rectal NSAIDs at doses of 20–25 mg and 50 mg appeared to prevent the progression of PEP to severe disease. To our knowledge, this is the first study to describe recent trends in ERCP and PEP since the late 2010s, as well as those in rectal NSAIDs and PIs. Our findings provide valuable insights into the evolving landscape of ERCP and PEP management in Japan.
This study revealed an increasing trend in ERCP procedures performed from FY 2016 to FY 2022. Notably, therapeutic ERCP accounted for 90% of all ERCP procedures. While the number of therapeutic ERCP increased, diagnostic ERCP showed a declining trend. These findings align with previous population-based studies in other countries, including the United States, Canada, South Korea, and China [5, 13, 26, 27]. One possible explanation for this trend is the growing prevalence of conditions requiring therapeutic ERCP, such as choledocholithiasis and pancreatobiliary cancers, driven by Japan’s rapidly aging population. These diseases commonly develop in individuals in their 70 s to 80 s [28, 29], and we also observed an upward trend in the age of patients undergoing ERCP. Another contributing factor may be the expansion of ERCP indications due to advances in techniques and devices [13]. The decrease in diagnostic ERCP is likely attributable to improved diagnostic accuracy and the widespread adoption of non-invasive modalities such as magnetic resonance cholangiopancreatography and endoscopic ultrasonography [5, 13, 30]. While a reduction in diagnostic ERCPs could lead to an overall decline in the total number of ERCP procedures, the factors driving an increase in ERCP procedures appear to have had a more pronounced impact in Japan in recent years.
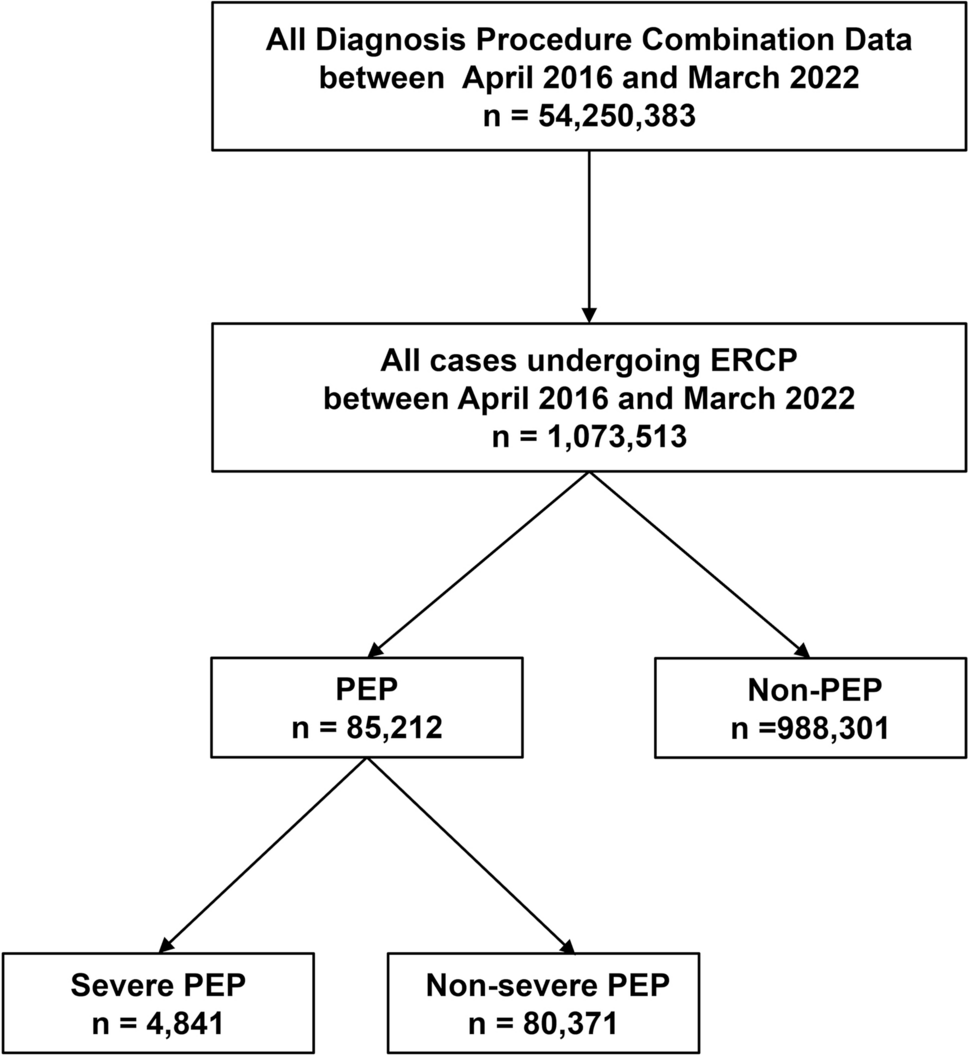
In this study, the incidence of PEP and severe PEP was 7.9% and 0.5%, respectively. These rates are consistent with those reported by Fujita et al. [31], who found similar incidences of 6.9% and 0.5% in a multicenter prospective study on ERCP-related adverse events in Japan. Recent population-based studies have also reported that the incidence of PEP ranges from 4.3 to 16.5% [6, 13, 27]. Many studies have shown an increasing trend in PEP incidence, likely due to the growing number of therapeutic ERCPs and the increasing complexity of cases requiring highly skilled interventions [6, 13]. However, in contrast to these findings, our study demonstrated a decreasing trend in PEP incidence. Several factors may explain this decline. First, preventive strategies for PEP have evolved significantly. Increasing evidence supports the effectiveness of rectal NSAIDs, aggressive hydration, and prophylactic pancreatic stents in preventing PEP [2, 3, 14]. The combined use of these measures has been shown to further reduce PEP risk [32, 33]. Second, the publication of the first clinical practice guidelines for PEP in 2015 [14], along with the revised guidelines for the management of AP in the same year [34], may have increased awareness of PEP risk factors and preventive strategies among Japanese endoscopists. Third, our study focused on the period from 2016 to 2023, whereas previous studies included data only up to 2017 at the latest. This more recent timeframe may better reflect the impact of updated clinical practices. Finally, ERCP in Japan is typically performed in an inpatient setting, which may facilitate the implementation of preventive measures. In contrast, ERCP is often conducted on an outpatient basis in other countries [35], potentially limiting the use of certain preventive strategies.
Our study found that the PEP-related mortality rate was 0.2% among PEP cases, which aligns with findings from a recent systematic review and meta-analysis [4]. Notably, based on our severity criteria, only 14.4% of fatal cases were classified as severe PEP. One possible explanation is that our criteria are stricter than the Japanese severity criteria. In the most recent nationwide epidemiological survey for acute pancreatitis (AP), the proportion of severe cases was similar between all AP cases (23.6%) and PEP cases (23.8%) [36]. However, in our previous study using the DPC database, 27.7% of all AP cases were classified as severe—significantly higher than the proportion of severe PEP cases (5.7%) in this study. This discrepancy suggests that cases classified as severe based on the Japanese criteria may have been categorized as non-severe under our criteria. Another important factor is the advanced age of PEP patients. The mean age of PEP cases in our study was 74.3 years, considerably older than the reported mean age of 61.4 years for all AP cases [19]. In elderly patients, even non-severe PEP may be life-threatening, particularly in those with comorbidities, including malignancies. In fact, malignancies were recorded as the primary disease in 31 (15.3%) of the fatal cases, and among them, 28 (90.3%) were classified as non-severe PEP. It is possible that aggressive treatment, typically indicated for severe cases, was not pursued in these patients due to the presence of malignancies. Unfortunately, for patients whose mortality was attributed to a condition other than the one requiring the highest utilization of medical resources, the exact cause of death remains unclear. We could not rule out that the exact cause of death was unrelated to PEP in these cases.
Several systematic reviews and meta-analyses have demonstrated the effectiveness of rectal NSAIDs in preventing PEP [4, 37, 38]. Accordingly, both the American Society for Gastrointestinal Endoscopy and the European Society of Gastrointestinal Endoscopy recommend their administration in all patients undergoing ERCP [2, 3]. However, in this study, it was unclear whether rectal NSAIDs were used prophylactically for PEP prevention or for pain relief after ERCP, as the DPC database does not provide information on the timing or purpose of their administration. Nevertheless, given the accumulation of recent evidence, the concurrent increase in rectal NSAIDs use, and the decline in PEP incidence, it is reasonable to infer that the increased use of rectal NSAIDs was primarily intended for PEP prevention. Interestingly, rectal NSAIDs use was identified as a factor associated with an increased incidence of PEP. This is likely due to selection bias, as rectal NSAIDs were more frequently administered to patients with high-risk backgrounds and procedural factors associated with PEP. Regarding the severity of PEP, a meta-analysis of eight studies reported that rectal NSAIDs significantly reduced the incidence of moderate-to-severe PEP (OR, 0.53; 95% confidence interval, 0.31–0.89) [39]. However, the preventive effect of low-dose rectal NSAIDs in severe PEP remains unclear. While a 100 mg dose is recommended in Western countries, lower doses (25–50 mg) are predominantly administered in Japan due to smaller body sizes and available dosage forms [40]. Our study revealed a decreasing trend in the incidence of severe PEP, along with an increasing trend in the use of low-dose rectal NSAIDs at doses of 20–25 mg and 50 mg. Furthermore, low-dose rectal NSAIDs use was identified as a factor associated with a lower incidence of severe PEP. To our knowledge, this is the first study to suggest the potential effectiveness of low-dose rectal NSAIDs (20–25 mg and 50 mg) in preventing the progression of PEP to severe disease.
In Japan, PIs have traditionally been used to prevent PEP. Using the public health insurance claims database of the Japan Medical Data Center, Seta et al. [24] reported that the use of PIs in patients undergoing ERCP increased from 72.3% in 2005–2007 to 83.6% in 2010–2015. In contrast, our study demonstrated a decreasing trend in PIs usage, from 70.5% in 2016–2017 to 53.5% in FY 2022. Although our study and Seta et al. [24] utilized different databases, PIs usage may have begun to decline around 2015. This shift may have been influenced by the publication of the Japanese clinical guidelines for PEP in 2015 [14] and the revised guidelines for the management of AP in the same year [34]. The revised AP guidelines explicitly state that drugs other than NSAIDs should not be routinely used for PEP prevention, as their efficacy has been refuted or remains uncertain. They also indicate that the effectiveness of intravenous PIs for AP has not been established. Following these revisions, a similar decline in PIs usage has been observed in AP management overall [19]. The implementation of clinical indicators, known as "pancreatitis bundles," has been associated with reduced mortality in patients with severe AP [41]. These findings highlight the significant impact of clinical guidelines on both decision-making and clinical outcomes. Most recently, the clinical practice guidelines for PEP were updated in 2023 [42], strongly recommending against the use of PIs for PEP prevention. It will be important to monitor whether the prophylactic use of PIs continues to decline in response to these updated recommendations.
This study has several limitations, primarily due to the nature of the DPC database. First, the diagnosis of PEP was based on recorded text data. Additionally, when mortality was attributed to a condition other than the one requiring the highest utilization of medical resources, the exact cause of death could not be determined. Second, the DPC database lacks detailed procedural information related to ERCP, including factors known to influence the risk of PEP, such as precut sphincterotomy, the number of cannulation attempts, and cannulation time. Moreover, it was not possible to determine whether the papilla of Vater was naïve or if the patient had previously undergone ERCP. The DPC database does not allow for patient tracking beyond the current hospitalization, limiting long-term follow-up. Third, medication use was at the discretion of the endoscopist, and information regarding the timing and purpose of rectal NSAIDs and PIs administration was unavailable. The higher usage rate of rectal NSAIDs in PEP cases and their identification as a risk factor for PEP may reflect selection bias, as NSAIDs were likely administered preferentially to high-risk patients. Finally, the database does not capture information on other preventive measures for PEP, such as prophylactic pancreatic stents and aggressive hydration. Despite these limitations, our study provides valuable insights into the current status and temporal trends of ERCP, PEP, and specific preventive measures in Japan.
In conclusion, while the number of ERCP procedures and the proportion of therapeutic ERCPs have been increasing in Japan, the incidences of PEP and severe PEP have shown a declining trend. The usage of rectal NSAIDs has increased, and low-dose rectal NSAIDs (20–25 mg and 50 mg) may help reduce PEP severity. These trends may have been influenced by the publication and implementation of clinical practice guidelines for PEP and AP.



Comments (0)