With an estimated annual incidence of 390 million infections worldwide, dengue is the most common arthropod-borne virus that infects humans. A quarter of these infections are symptomatic [1]. Most cases are self-limited, but one in 20 patients with dengue in the United States of America develop severe disease [2]. Over the past decade, the incidence of dengue infection has increased rapidly due to population growth in endemic areas. An estimated sixty per cent of the world’s population could be at risk of dengue infection by 2080 [1]. According to the National Centre for Vector-Borne Disease Control (NCVBDC), there has been steady growth in the annual incidence of dengue in India, with 233,251 cases documented in 2022, rising to 289,000 in 2023 [3].
According to the Intergovernmental Panel on Climate Change (IPCC), climate change facilitates the expansion of vectors and vector-borne diseases, such as dengue, to higher altitudes and latitudes, globalizing the disease. Given the inverse relationship between temperature and elevation, global warming is expected to transform high-altitude ecosystems to resemble those at lower altitudes. In many mountainous regions, glaciers are receding, and cooler-temperature plant species have migrated to higher elevations [4]. Changes in fauna accompany these flora shifts. In Mexico, the first recorded instances of dengue fever at an altitude of 1700 m occurred during an unusually warm summer in 1988 [4]. Changes in the geographic distribution and intensity of malaria and dengue transmission due to future climate change may significantly increase the risk among the immunologically naïve global population and overall disease. Dengue fever is particularly sensitive to climatic variations, with optimal transmission at 27 to 35 degrees Celsius. Meteorological conditions affect mosquito longevity, parity, fecundity, gonotrophic cycle, and incubation periods, influencing disease transmission. Temperature and humidity impact dengue by affecting larval development, adult feeding behaviour, and mosquito survival, while rainfall creates breeding habitats. However, excessive rainfall can disrupt breeding sites, leading to varied associations between rainfall and dengue incidence [5,6,7,8,9].
The strain of the virus, the host immune response, and genetic factors play vital roles in disease pathogenesis and severity. Severe dengue is noted to have increased plasma leakage and abnormal haemostasis. An uncontrolled inflammatory response with high ferritin levels is a rare complication of dengue. Recent studies have shown that ferritin is a valuable marker for inflammation in dengue [10].
Haemophagocytic lymphohistiocytosis (HLH) is a life-threatening monocyte/ macrophage-related histiocytic disorder. There are familial and sporadic variants of this disease. It is characterised by hyperinflammation, which can cause cytopenia(s), splenomegaly, hepatitis, and central nervous system dysfunction. Farquhar and Claireux first described HLH in 1952 as a familial disease [11]. Identifying HLH is challenging because of its overlapping features with other inflammatory disorders, hence the need for a simple diagnostic clinical tool. Thus, the exact incidence and prevalence of HLH are challenging to determine but are estimated to occur in 1 in 2000 adult admissions in tertiary care centres [12].
Sporadic HLH, previously referred to as secondary HLH, is triggered by infection, malignancy, rheumatologic disorders, immune-activating therapies, and immune suppression. Infections such as Ebstein-Barr virus (EBV), influenza virus, cytomegalovirus (CMV), and in endemic areas, dengue, malaria, toxoplasmosis, and leishmaniasis can trigger HLH [12].
According to recent studies, 3.12% of patients with dengue fever develop HLH, which increases to 10 − 22.1% in severe dengue [13]. In dengue-associated HLH, dengue infection triggers macrophage activation, leading to cytokine storm and immune-mediated tissue destruction [13, 14]. Mortality in dengue-associated HLH patients is reported to be as high as 20.2% [13].
Fever, cytopenia(s), hepatomegaly, hepatitis and hyperferritinaemia occur both in severe dengue and HLH patients. In addition to these features, patients with HLH have prolonged fever (lasting more than seven days), splenomegaly, elevated lactate dehydrogenase (LDH) and triglyceride levels, hypofibrinogenaemia and haemophagocytosis [15]. A high degree of clinical suspicion is required to diagnose HLH in the setting of severe dengue.
The H-score is used to diagnose secondary HLH in dengue patients and includes parameters such as ferritin, triglycerides, liver enzymes, and fibrinogen [16]. A complete battery of these tests, including ferritin and CD-25, is expensive and inaccessible in resource-limited settings. To effectively screen patients for HLH, it is prudent to utilise a clinical tool, which leads to a high pretest probability for definitive tests and low false negative results.
A recent study has shown that the soluble IL-2 receptor (sIL-2R), which corresponds to T-cell activation, is a better predictor of HLH than serum ferritin, which is regularly used as one of the key markers to diagnose HLH [17].
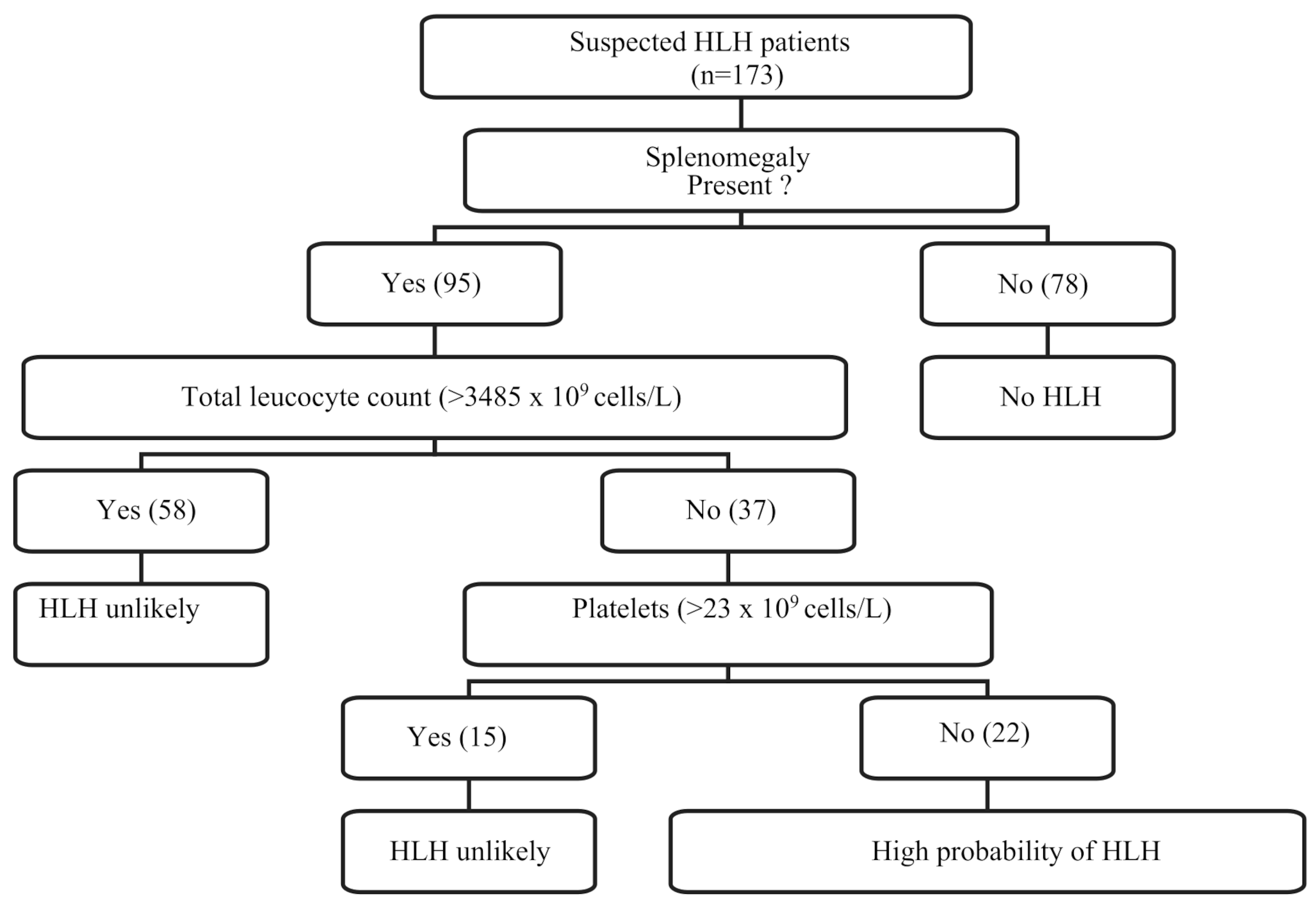
This study aims to develop a simplified clinical tool that formulates specific criteria for screening dengue patients for HLH. This tool aims to ensure that hospital resources are utilised effectively and reduce the financial burden on the patients, who could otherwise not afford a comprehensive set of diagnostic tests in resource-limited settings.


Comments (0)